
Int J Curr Pharm Res, Vol 17, Issue 2, 26-29Original Article
EVALUATION OF THE SAFETY AND EFFICACY OF SUPRACLAVICULAR BLOCK COMBINED WITH SUPERFICIAL CERVICAL BLOCK FOR SHOULDER SURGERY
SUMAN KUMARI DABI, SANJAY KUMAR MEENA, SUBHASREE N, LAKSHMI R.*
Department of Anaesthesia, AIIMS, New Delhi, India
*Corresponding author: Lakshmi R.; *Email: mail2lakshmi1991@gmail.com
Received: 13 Dec 2024, Revised and Accepted: 24 Feb 2025
ABSTRACT
Objective: Regional anaesthesia techniques, such as supraclavicular block combined with superficial cervical block, have gained popularity for shoulder surgeries due to their efficacy and safety profile. This study evaluates the onset, duration, and complications associated with this anaesthesia technique in patients undergoing upper arm surgery.
Methods: A descriptive observational study was conducted on 150 patients aged 15-65 y, classified as ASA grade I and II, undergoing upper arm surgery at S. M. S. Medical College and attached group of Hospitals, Jaipur, between January 1, 2019, and June 30, 2019. Patients with diabetes mellitus, neurological deficits, coagulopathy, or those who refused participation were excluded. Anesthetic block characteristics were recorded, and patients were monitored for any complications.
Results: The mean onset time for sensory block was 7.64±1.34 min, and for motor block, it was 10.93±2.08 min. The duration of analgesia averaged 996.53±129.23 min, while the motor block lasted for 850.41±52.94 min. Out of 150 patients, 91 were ASA grade III, and 59 were ASA grade IV. No clinical complications such as nausea, vomiting, difficulty in breathing, local anesthetic systemic toxicity, clinical pneumothorax, or Horner's syndrome were observed.
Conclusion: The combination of supraclavicular block and superficial cervical block is a safe and effective anaesthesia technique for shoulder surgeries, offering rapid onset and prolonged analgesia with minimal complications.
Keywords: Supraclavicular block, Superficial cervical block, Shoulder surgery, Regional anaesthesia, Anesthetic complications
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i2.6045 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Shoulder surgeries, ranging from arthroscopic procedures to total shoulder replacements, present unique challenges in terms of anaesthesia and postoperative pain management. Effective anaesthesia is crucial not only for the success of the surgery but also to ensure patient comfort and facilitate early recovery [1, 2]. Traditional approaches often rely on general anaesthesia, which, while effective, comes with its own set of complications such as nausea, vomiting, and a longer recovery period [1]. In response to these challenges, regional anaesthesia techniques have gained popularity due to their ability to provide targeted pain relief with fewer systemic effects [3].
The supraclavicular block, a regional anaesthesia technique, targets the brachial plexus at the level of the trunks. This approach effectively anesthetizes the upper limb, making it a suitable choice for surgeries involving the shoulder and upper arm [2, 4]. By depositing local anesthetic near the nerve roots, it ensures a dense blockade, suitable for complex procedures. The benefits of this technique include a rapid onset of action, consistent results, and the avoidance of the side effects commonly associated with general anaesthesia [5].
However, shoulder surgeries often require not only a blockade of the nerves servicing the upper limb but also those that provide sensory input to the shoulder area itself. This is where the addition of a superficial cervical block can be advantageous. This block anesthetizes the superficial cervical plexus, covering the cutaneous nerves that supply the skin over the shoulder area [6, 7]. When combined with a supraclavicular block, it enhances analgesia in the shoulder region, which can be particularly beneficial for patients undergoing extensive surgical procedures.
This study aims to evaluate the safety and efficacy of combining the supraclavicular block with a superficial cervical block for shoulder surgeries. The objectives are to assess the onset times of the blocks, the duration of analgesia they provide, and any potential complications associated with this dual-block technique. By comparing these outcomes with those of general anaesthesia or a single block approach, the study seeks to provide evidence on whether the combined approach could be considered a superior method for managing anaesthesia in shoulder surgery [8-10].
The significance of this research lies in its potential to contribute to the optimization of anaesthesia techniques for shoulder surgeries. With an increasing number of these procedures being performed each year, improving the quality of analgesia while reducing the risk of complications could have a substantial impact on clinical practices and patient outcomes. Moreover, this study could help refine anaesthesia protocols, leading to more personalized and effective pain management strategies for patients undergoing shoulder surgeries.
MATERIALS AND METHODS
Study design and setting
A descriptive observational study was conducted in the Trauma Operating Theatre under the Department of Anaesthesia at S. M. S. Medical College and attached group of Hospitals, Jaipur. The study period spanned from January 1, 2019, to June 30, 2019, following approval from the Institutional Ethical Committee.
Sample size
A total of 150 patients scheduled for upper arm surgery were included in the study during the specified period.
Inclusion criteria
Age between 15 and 65 y
Patients undergoing upper arm surgery
Classified as American Society of Anesthesiologists (ASA) grade I or II
Exclusion criteria
History of diabetes mellitus
Presence of neurological deficits
Coagulopathy disorders
Refusal to participate in the study
Anesthetic technique
All patients received a combination of supraclavicular block and superficial cervical block. The blocks were performed under sterile conditions with standard monitoring of vital signs. The onset of sensory and motor blocks was assessed every 2 min until complete blockade was achieved. The duration of analgesia and motor block was recorded.
Data collection and statistical analysis
Continuous variables such as age, blood pressure, heart rate, and time were presented as mean±standard deviation (SD). Categorical variables like ASA grade were presented as frequencies and percentages and analyzed using the Chi-Square test. Statistical significance was considered at p < 0.05.
RESULTS
Anesthetic block characteristics
The onset and duration of sensory and motor blocks are summarized in table 1.
Table 1: Anesthetic block characteristics
| Parameter | Mean | SD |
| Onset of sensory block (min) | 7.64 | ±1.34 |
| Duration of analgesia (min) | 996.53 | ±129.23 |
| Onset of motor block (min) | 10.93 | ±2.08 |
| Duration of motor block (min) | 850.41 | ±52.94 |
Patient distribution by ASA grade
Out of 150 patients, 91 were classified as ASA grade III, and 59 as ASA grade IV (table 2).
Clinical complications observed
No clinical complications were observed in any of the patients (table 3).
Table 2: Patient distribution by ASA grade
| ASA grade | Number of patients |
| III | 91 |
| IV | 59 |
| Total | 150 |
Table 3: Clinical complications observed
| Complication | Number of patients |
| Nausea | Nil |
| Vomiting | Nil |
| Difficulty in breathing | Nil |
| Local anesthetic systemic toxicity | Nil |
| Clinical pneumothorax | Nil |
| Horner's syndrome | Nil |
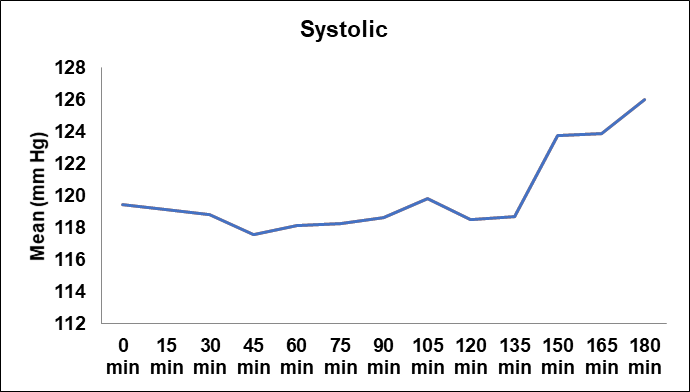
Fig. 1: Trend of mean systolic blood pressure over time
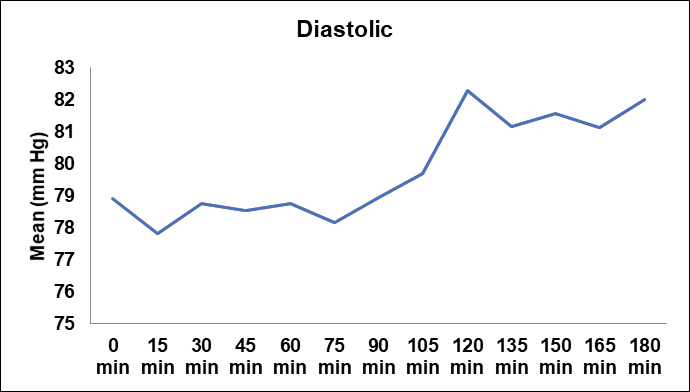
Fig. 2: Trend of mean diastolic blood pressure over time
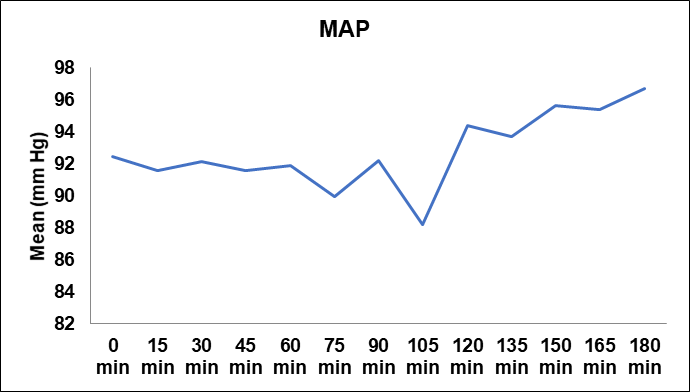
Fig. 3: Trend of mean arterial pressure (map) over time
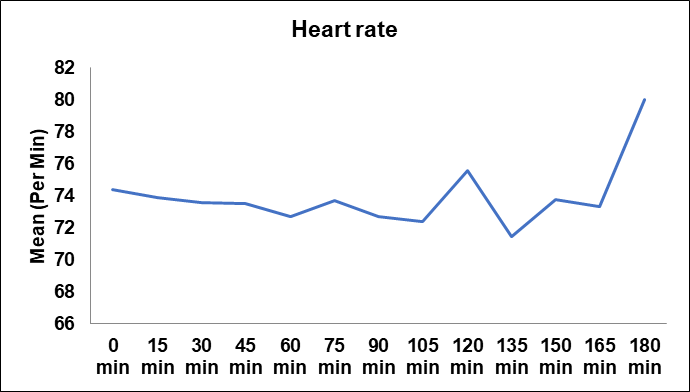
Fig. 4: Heart rate fluctuations over time
DISCUSSION
The integration of supraclavicular and superficial cervical blocks in shoulder surgeries has proven to be a highly effective anaesthesia strategy. This study's findings revealed that the dual-block technique not only facilitates a rapid onset of both sensory and motor blocks but also extends the duration of analgesia significantly. The average onset time recorded for the sensory block was 7.64±1.34 min and for the motor block was 10.93±2.08 min, demonstrating a swift establishment of anaesthesia which is critical in maintaining surgical schedules and enhancing patient throughput in busy surgical centers [11].
Furthermore, the prolonged duration of analgesia, averaging approximately 16.6 h, indicates that this technique provides sustained postoperative pain relief. This is a significant improvement over traditional methods, as it substantially reduces the reliance on systemic analgesics, which are often associated with side effects such as opioid-induced respiratory depression and constipation [12-15]. By limiting the need for additional pain medication post-surgery, patients can experience a more comfortable recovery and a potentially lower risk of complications associated with opioid use.
The safety profile observed in this study further strengthens the case for the routine use of this combined block technique in shoulder surgeries. Notably, the absence of complications such as nausea, vomiting, respiratory difficulties, systemic toxicity, pneumothorax, and Horner's syndrome is particularly encouraging. These results align with existing literature on regional anaesthesia, which consistently reports lower incidence rates of such complications compared to general anaesthesia, thereby supporting broader adoption of regional blocks in clinical practice [14, 16].
Comparatively, the findings from previous studies suggest that while single-block techniques are effective, they do not provide the same level of comprehensive sensory and motor nerve coverage as the combined approach. This can lead to patchy or insufficient analgesia, necessitating supplementary systemic analgesics and exposing patients to additional risks. The dual-block technique addresses this gap effectively, offering a more reliable and complete anaesthesia solution specifically tailored for the complexities of shoulder surgeries.
The implications of these findings are significant for anesthetic practice. They suggest that anesthesiologists should consider adopting the combined supraclavicular and superficial cervical block technique more widely, especially for procedures known for their postoperative pain challenges. Additionally, these results may prompt further research into optimizing local anesthetic concentrations and volumes to maximize the efficacy and safety of the blocks, potentially leading to refined protocols that could set new standards in regional anaesthesia for shoulder surgeries [17].
In conclusion, the combination of supraclavicular and superficial cervical blocks represents a superior anaesthesia method for shoulder surgeries characterized by rapid onset, prolonged analgesia, and an excellent safety profile. This study not only corroborates previous research but also provides compelling evidence to support the expanded use of this technique in clinical settings.
CONCLUSION
Supraclavicular block combined with superficial cervical block is a safe and effective anaesthesia method for shoulder surgeries, offering rapid onset of anaesthesia and prolonged postoperative analgesia with minimal risk of complications. This technique can be considered a valuable option in the anesthetic management of patients undergoing upper arm surgeries.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCES
Hadzic A, Williams BA, Karaca PE, Hobeika P, Unis G, Dermksian J. For outpatient rotator cuff surgery nerve block anesthesia provides superior same-day recovery over general anesthesia. Anesthesiology. 2005;102(5):1001-7. doi: 10.1097/00000542-200505000-00020, PMID 15851888.
Brown AR, Weiss R, Greenberg C, Flatow EL, Bigliani LU. Interscalene block for shoulder arthroscopy: comparison with general anesthesia. Arthroscopy. 1993;9(3):295-300. doi: 10.1016/s0749-8063(05)80425-6, PMID 8323615.
Jadon A, Sharma M, Pandey R, Sinha N, Chakraborty S. A comparative study of ultrasound-guided supraclavicular brachial plexus block with or without dexmedetomidine as an adjuvant to local anesthetics. Indian J Pain. 2014;28(3):155-9.
Bromage PR. Damage to the conus medullaris following spinal anaesthesia: 1. Anaesthesia. 2001;56(8):812-3. doi: 10.1046/j.1365-2044.2001.02181-22.x, PMID 11494419.
Gauss A, Mayer G, Cunitz G, Weindel M. Continuous interscalene brachial plexus block versus general anaesthesia in shoulder surgery. J Clin Anesth. 1991;3(1):33-6.
Koscielniak Nielsen ZJ. Ultrasound-guided peripheral nerve blocks: what are the benefits? Acta Anaesthesiol Scand. 2008;52(6):727-37. doi: 10.1111/j.1399-6576.2008.01666.x, PMID 18477070.
Kothari D. Supraclavicular brachial plexus block: a new approach. Indian J Anaesth. 2003;47(4):287-8.
Williams SR, Chouinard P, Arcand G, Harris P, Ruel M, Boudreault D. Ultrasound guidance speeds execution and improves the quality of supraclavicular block. Anesth Analg. 2003;97(5):1518-23. doi: 10.1213/01.ANE.0000086730.09173.CA, PMID 14570678.
Khanna P, Ray BR, Govindrajan SR, Sinha R, Chandralekha, Talawar P. Anesthetic management of pediatric patients with sturge weber syndrome: our experience and a review of the literature. J Anesth. 2015;29(6):857-61. doi: 10.1007/s00540-015-2042-8, PMID 26194909.
Tran DQ, Russo G, Munoz L, Zaouter C, Finlayson RJ. A prospective randomized comparison between single and double injection ultrasound-guided supraclavicular block. Reg Anesth Pain Med. 2010;35(1):16-21.
Ilfeld BM, Morey TE, Wright TW, Chidgey LK, Enneking FK. Continuous interscalene brachial plexus block for postoperative pain control at home: a randomized double-blinded placebo-controlled study. Anesth Analg. 2003;96(4):1089-95. doi: 10.1213/01.ANE.0000049824.51036.EF, PMID 12651666.
Chan VW, Perlas A, Rawson R, Odukoya O. Ultrasound-guided supraclavicular brachial plexus block. Anesth Analg. 2003;97(5):1514-7. doi: 10.1213/01.ANE.0000062519.61520.14, PMID 14570677.
Marhofer P, Greher M, Kapral S. Ultrasound guidance in regional anaesthesia. Br J Anaesth. 2005;94(1):7-17. doi: 10.1093/bja/aei002, PMID 15277302.
Abrahams MS, Aziz MF, FU RF, Horn JL. Ultrasound guidance compared with electrical neurostimulation for peripheral nerve block: a systematic review and meta-analysis of randomized controlled trials. Br J Anaesth. 2009;102(3):408-17. doi: 10.1093/bja/aen384, PMID 19174373.
Liu SS, Ngeow JE, Yadeau JT. Ultrasound-guided regional anesthesia and analgesia: a qualitative systematic review. Reg Anesth Pain Med. 2009;34(1):47-59. doi: 10.1097/AAP.0b013e3181933ec3, PMID 19258988.
Winnie AP, Ramamurthy S, Durrani Z, Radonjic R. Interscalene cervical plexus block: a single injection technic. Anesth Analg. 1975;54(3):370-5. doi: 10.1213/00000539-197505000-00030, PMID 1169028.
Kang CM, Kim MS, Hwang BM. Comparison of ultrasound-guided superficial cervical plexus block versus intermediate cervical plexus block for thyroid surgery. Anesthesiol Pain Med. 2019;14(2):164-70.