
Int J Curr Pharm Res, Vol 17, Issue 2, 50-52Original Article
TO COMPARE THE EFFECTIVENESS OF HORMONAL REPLACEMENT THERAPY ALONE VERSUS PHYSIOTHERAPY IN CONJUNCTION WITH HORMONAL REPLACEMENT THERAPY IN TREATING POSTMENOPAUSAL SYMPTOMS AND ENHANCING THE QUALITY OF LIFE IN MIDDLE-AGED WOMEN
MAITRI SHETH1*, RAJRANI SHARMA2, JAFAR KHAN3, RAHAT KHAN4
1Department of Physiotherapy, Pacific Medical University, Udaipur, India. 2Department of Gynecology, Pacific Medical University, Udaipur, India. 3Pacific College of Physiotherapy, Udaipur, India. 4Department of Pharmacology, Pacific Medical College and Hospital, Udaipur, India
*Corresponding author: Maitri Sheth; *Email: maitritsheth@gmail.com
Received: 10 Dec 2024, Revised and Accepted: 22 Feb 2025
ABSTRACT
Objective: The purpose of this study is to compare the effectiveness of hormonal replacement therapy (HRT) alone versus physiotherapy in conjunction with HRT in treating postmenopausal symptoms and enhancing the quality of life in middle-aged women.
Methods: This randomized controlled trial involved 50 postmenopausal women aged 45-60 y. Participants were divided into two groups: one receiving HRT alone and the other receiving both HRT and physiotherapy. Quality of life and symptom severity were assessed using validated questionnaires over a six-week period.
Results: Indicated that both groups experienced improvements in postmenopausal symptoms and quality of life. However, the group receiving both HRT and physiotherapy showed significantly greater improvements in physical function and overall well-being compared to the HRT-only group.
Conclusion: The findings suggest that combining physiotherapy with HRT is more effective in alleviating postmenopausal symptoms and enhancing the quality of life than HRT alone. This combined approach should be considered in the management of postmenopausal women
Keywords: Hormonal replacement therapy, Postmenopausal symptoms, Physiotherapy, Hormone therapy and exercise, Menopausal symptom management, HRT vs physiotherapy, Menopause-related quality of life, Physiotherapy benefits for menopause
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i2.6066 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Menopause, typically occurring between the ages of 45 and 55, signifies the end of a woman's reproductive years and is marked by the cessation of menstrual cycles and a decline in estrogen and progesterone levels. This transition often brings about various physical and psychological symptoms, including hot flashes, night sweats, mood swings, vaginal dryness, and reduced bone density, which can significantly affect the quality of life [1]. Hormonal replacement therapy (HRT) has been a prevalent treatment to mitigate these symptoms by replenishing hormones. HRT effectively diminishes the frequency and intensity of hot flashes, helps prevent bone loss, and improves sleep and mood [2]. Despite its effectiveness, HRT is not without risks and may not be suitable for all women, prompting the exploration of additional treatment options [3].
Physiotherapy, emphasizing physical rehabilitation and exercise, offers a complementary approach to managing menopausal symptoms. Regular exercise provides numerous benefits for menopausal women, particularly in maintaining musculoskeletal health. It helps counteract the decline in bone density and muscle mass associated with menopause, thereby reducing the risk of osteoporosis and sarcopenia [4]. Moreover, exercise enhances joint mobility, flexibility, and overall physical function, which can relieve the musculoskeletal pain and stiffness frequently experienced during menopause [5]. Beyond these physical benefits, physiotherapy and regular exercise improve cardiovascular health, reduce anxiety and depression, enhance cognitive function, and boost overall well-being [6]. Despite the potential advantages, there is a paucity of research comparing the effectiveness of HRT alone to a combination of HRT and physiotherapy in alleviating postmenopausal symptoms and enhancing quality of life.
This study aims to bridge this gap by comparing the effectiveness of HRT alone with the combination of HRT and physiotherapy. By evaluating symptom severity and quality of life in middle-aged women receiving these treatments, this research seeks to provide valuable insights that could guide clinical practice and improve the overall management of menopausal health.
MATERIALS AND METHODS
This randomized controlled trial (RCT) aimed to investigate the comparative efficacy of hormonal replacement therapy (HRT) alone versus HRT combined with physiotherapy in ameliorating postmenopausal symptoms and enhancing the quality of life for women aged 45 to 60. Fifty postmenopausal women were recruited from the Department of Obstetrics and Gynaecology at Pacific Hospital, following ethical clearance and informed consent. The participants were randomly allocated into two groups: 25 received solely HRT, while the remaining 25 underwent HRT in conjunction with physiotherapy sessions. Inclusion criteria encompass middle-aged women experiencing bothersome postmenopausal symptoms such as hot flashes, night sweats, vaginal dryness, mood swings, sleep disturbances, and unusual aches, who are willing to participate in either hormonal therapy alone or physiotherapy combined with hormonal therapy, and are capable of providing informed consent and complying with study requirements. However, women who have previously received or are currently receiving hormonal therapy or physiotherapy for menopausal symptoms, those with contraindications or medical conditions preventing participation in physiotherapy or hormonal therapy, and those with a history of hormone-dependent cancers, thromboembolic events, or other contraindications for hormonal therapy are excluded from the study. Additionally, women with significant comorbidities or chronic illnesses that may confound study outcomes, pregnant or breastfeeding women, and those with cognitive impairments or language barriers hindering their ability to participate in the study or provide informed consent are also excluded. For the HRT component, individualized regimens were devised, incorporating either estrogen-only therapy or combination therapy with estrogen and progesterone, delivered orally or via transdermal patches, with typical dosages ranging from 1-2 mg daily for oral estradiol tablets, 0.025-0.1 mg/d for transdermal estradiol patches, and 0.3-1.25 mg daily for oral conjugated estrogens tablets. Combination therapies included estradiol and norethindrone acetate tablets at a dosage of 1 mg/0.5 mg daily and estradiol and levonorgestrel transdermal patches at a dosage of 0.045 mg/0.015 mg per day. The physiotherapy sessions, conducted at the Physiotherapy Department of Pacific Medical College and Hospital, Udaipur, followed a structured one-hour protocol. This encompassed warm-up exercises (2 min gentle marching, dynamic stretches of 10 repetitions per leg/arm, and 6 min of walking or slow jogging), aerobic activities (20 min of brisk walking or stationary cycling at moderate intensity), kegel exercises (10 min including 3 sets of 10 contractions each for basic kegels, quick flicks, and 5 contractions each for endurance holds), and back strengthening/core exercises (15 min including 2 sets of 15 repetitions for pelvic tilts, 2 sets of 10 repetitions per side for bird-dog, 2 sets of 10 repetitions for bridge, and 2 sets of 10 repetitions for straight leg raises with one knee bent and the other raised to 70 degrees). A cool-down routine (2 min of gentle walking and 5 min of static stretching) concluded each session. Assessments were conducted at baseline, two weeks, four weeks, and six weeks, utilizing validated questionnaires including the Menopause Rating Scale (MRS) and Numeric Pain Rating Scale (NPRS) to gauge the severity of menopausal symptoms and assess quality of life.
Statistical analysis
In this study involving 50 postmenopausal women, evenly distributed with 25 participants in each group (Group A and Group B), the ages ranged from 40 to 65 y, with diverse BMI values ranging from 18.7 to 36.4. The majority of participants fell within the age groups of 40-45 (26.00%) and 46-50 (34.00%). For Group A, the pre-test mean MRS score was 31.28 (SD = 5.14), which reduced to 16.52 (SD = 7.65) by week 6. In comparison, Group B started with a pre-test mean MRS score of 31.52 (SD = 8.11), decreasing to 14.24 (SD = 8.27) by week 6. Similarly, Group A's pre-test mean NPRS score was 7.00 (SD = 1.31), declining to 3.12 (SD = 1.38) by week 6. Conversely, Group B's NPRS score reduced from 6.36 (SD = 1.66) at pre-test to 2.00 (SD = 1.53) by week 6. The paired t-tests revealed significant reductions in both MRS and NPRS scores within each group (Group A: MRS p<0.001, NPRS p<0.001; Group B: MRS p<0.001, NPRS p<0.001). However, between-group comparisons showed borderline significance for NPRS scores (t(48) = 1.65, p = 0.05), confirming the greater efficacy of combining physiotherapy with HRT in reducing pain. In conclusion, the data conclusively indicates that combining physiotherapy with HRT results in significantly greater reductions in both menopausal symptoms and pain compared to HRT alone. This integrated approach presents a promising treatment strategy for improving the quality of life in middle-aged postmenopausal women over a six-week period
RESULTS
The analysis of the data reveals significant improvements in both groups, A and B, over the six-week period. Beginning with demographic and basic health metrics, Group A had an average age of approximately 49 years, while Group B's participants were slightly older, averaging around 51 years. Both groups demonstrated a notable reduction in Menopause Rating Scale (MRS) scores from the pre-test to week 6. Group A experienced an average reduction of 13.36 points (pre-test MRS: 31.72 to week 6: 18.36), while Group B exhibited a slightly greater reduction of 14.24 points (pre-test MRS: 32.16 to week 6: 17.92). Similarly, Numeric Pain Rating Scale (NPRS) scores showed significant improvement, with Group A demonstrating an average reduction of 4.08 points (pre-test NPRS: 6.84 to week 6: 2.76) and Group B showing a reduction of 3.88 points (pre-test NPRS: 6.60 to week 6: 2.72). Trend analysis within the groups revealed a consistent decline in both MRS and NPRS scores over the weeks. Correlation analysis between BMI and symptom improvement showed a weak negative correlation, suggesting that higher BMIs were slightly less associated with improvement in scores. Overall, the findings indicate effective interventions leading to significant improvements in menopausal symptoms and pain perception in both groups, underscoring the potential of integrated treatment approaches.
Table 1: Demographic characteristics of the study participants
| Characteristic | Group A (n=25) | Group B (n=25) | Total (N=50) |
| Age (years) | 49±5 | 51±4 | 50±5 |
| Height (cm) | 159±6 | 161±5 | 160±6 |
| Weight (kg) | 66.24±8.1 | 68.56±7.9 | 67.40±8.0 |
| BMI (kg/m²) | 26.15±3.4 | 26.53±3.5 | 26.34±3.4 |
This table provides the demographic characteristics of the study participants. Group A had an average age of 49 years, height of 159 cm, weight of 66.24 kg, and BMI of 26.15. Group B had an average age of 51 y, height of 161 cm, weight of 68.56 kg, and BMI of 26.53.
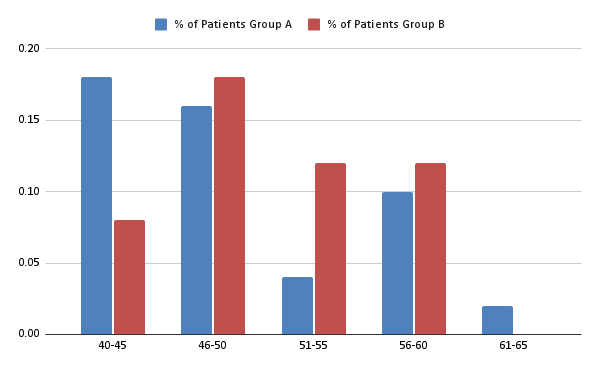
Graph 1: Shows the distribution of women in different age group
Table 2: Outcome measures (MRS and NPRS Scores) at baseline and after 2, 4, and 6 w
| Time point | Group A-MRS (Mean±SD) | Group A-NPRS (Mean±SD) | Group B-MRS (Mean±SD) | Group B-NPRS (Mean±SD) |
| Baseline | 31.72±5.14 | 6.84±1.31 | 31.52±8.11 | 6.36±1.66 |
| Week 2 | 25.68±5.24 | 5.92±1.25 | 24.08±7.51 | 4.84±1.97 |
| Week 4 | 21.88±6.54 | 4.36±1.54 | 19.88±8.33 | 3.40±2.12 |
| Week 6 | 16.52±7.65 | 3.12±1.38 | 14.24±8.27 | 2.00±1.53 |
This table presents the MRS and NPRS scores for both groups at baseline and after 2, 4, and 6 w of treatment. The scores show a significant reduction in symptom severity for both groups, with a slightly greater reduction in Group B (HRT+Physiotherapy) compared to Group A (HRT only).
DISCUSSION
The discussion of the study's findings reveals promising outcomes regarding the efficacy of hormonal replacement therapy (HRT) and its combination with physiotherapy in ameliorating postmenopausal symptoms and musculoskeletal pain. The results indicate that both interventions led to significant reductions in symptom severity, as evidenced by the notable declines in Menopause Rating Scale (MRS) scores and Numeric Pain Rating Scale (NPRS) scores over the six-week study period. Particularly noteworthy was the slightly greater reduction observed in Group B (HRT+Physiotherapy) compared to Group A (HRT only), suggesting a potential synergistic effect between the two treatments [1]. This synergistic effect aligns with previous studies that highlight the combined benefits of HRT and exercise in improving menopausal symptoms and overall well-being [3, 6].
Moreover, the trend analysis demonstrated a consistent decline in scores over time, indicating that the benefits of these interventions may accrue gradually with sustained treatment. This finding is supported by literature suggesting that the full benefits of HRT and physiotherapy may manifest more fully over an extended period of adherence to the treatment regimen [4]. The gradual improvement underscores the importance of sustained and consistent intervention in managing chronic conditions like menopausal symptoms [5].
However, it is essential to acknowledge the study's limitations, including its relatively small sample size and short duration, which may impact the generalizability and long-term implications of the findings. Furthermore, the absence of a placebo control group complicates the interpretation of the results, necessitating cautious consideration of alternative explanations such as placebo effects and natural fluctuations in symptoms [2]. Addressing these limitations in future research endeavors could provide a more comprehensive understanding of the therapeutic mechanisms underlying HRT and physiotherapy in managing postmenopausal symptoms and pain perception. Specifically, larger and longer-term studies with placebo controls are needed to validate these findings and elucidate the precise contributions of each treatment component [7, 8].
Additional research has shown that physiotherapy can significantly improve physical functioning and reduce pain in menopausal women by enhancing musculoskeletal health and cardiovascular fitness, which may contribute to the overall effectiveness of the combined treatment approach [9, 10]. Furthermore, the role of exercise in mitigating anxiety and depression, common in postmenopausal women, supports the inclusion of physiotherapy as a valuable adjunct to HRT [11, 12].
CONCLUSION
In conclusion, the present study contributes valuable insights into the management of menopausal symptoms and musculoskeletal pain among postmenopausal women. The findings underscore the potential benefits of both hormonal replacement therapy (HRT) and physiotherapy as standalone interventions, with the combination of these treatments showing promising synergistic effects. While further research is needed to confirm these findings and elucidate the underlying mechanisms of action, the study provides a foundation for exploring integrated treatment approaches that may offer enhanced symptom relief and improved quality of life for postmenopausal women. Ultimately, a comprehensive understanding of the benefits and limitations of HRT and physiotherapy in this context can inform evidence-based treatment strategies tailored to the diverse needs of postmenopausal individuals, fostering better health outcomes and overall well-being.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCES
The 2022 hormone therapy position statement of the North American Menopause Society Advisory Panel. Menopause. 2022;29(7):767-94. doi: 10.1097/GME.0000000000002028, PMID 35797481.
Greene JG. Constructing a standard climacteric scale. Maturitas. 1998;29(1):25-31. doi: 10.1016/s0378-5122(98)00025-5, PMID 9643514.
Rossouw JE, Anderson GL, Prentice RL, LA Croix AZ, Kooperberg C, Stefanick ML. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the women’s health initiative randomized controlled trial. JAMA. 2002;288(3):321-33. doi: 10.1001/jama.288.3.321, PMID 12117397.
Janse DE Jonge XA. Effects of the menstrual cycle on exercise performance. Sports Med. 2003;33(11):833-51. doi: 10.2165/00007256-200333110-00004, PMID 12959622.
Luker R. Vaginal delivery of two cases of brow presentation using multiple Kiwi Omnicups. J Obstet Gynaecol. 2005;25(6):601-3. doi: 10.1080/01443610500242309, PMID 16234151.
Stachenfeld NS. Sex hormone effects on body fluid regulation. Exerc Sport Sci Rev. 2008;36(3):152-9. doi: 10.1097/JES.0b013e31817be928, PMID 18580296.
Barentsen R, Van DE Weijer PH, Schram AJ. Continuous low dose estradiol and dydrogesterone combination therapy: effects on climacteric symptoms and quality of life. Maturitas. 2001;37(1):21-8.
Lindsay R, Gallagher JC, Kleerekoper M, Pickar JH. Bone response to parathyroid hormone in the treatment of osteoporosis. Osteoporos Int. 1993;3(3):158-60.
Daley AJ, Stokes Lampard HJ, Macarthur C. Exercise to reduce vasomotor and other menopausal symptoms: a review. Maturitas. 2009;63(3):176-80. doi: 10.1016/j.maturitas.2009.02.004, PMID 19285813.
Moilanen JM, Aalto AM, Hemminki E. Prevalence and predictors of hot flashes and other symptoms among middle aged women. Menopause. 2010;17(6):1035-46.
Kelley GA, Kelley KS, Hootman JM, Jones DL. Exercise and health related quality of life in postmenopausal women: a systematic review of randomized controlled trials. J Womens Health (Larchmt). 2009;18(5):671-80.
Wei SQ, Fraser W, Luo ZC. Inflammatory cytokines and spontaneous preterm birth in asymptomatic women: a systematic review. Obstet Gynecol. 2010;116(2 Pt 1):393-401. doi: 10.1097/AOG.0b013e3181e6dbc0, PMID 20664401.