
Int J Curr Pharm Res, Vol 17, Issue 2, 75-78Original Article
A CLINICOPATHOLOGICAL STUDY OF THE ENDOMETRIUM-DECIPHERING PATTERNS OF ABNORMAL UTERINE BLEEDING
K. T. ATHULYA KRISHNA KUMAR1*, KRISHNARAJ UPADHYAYA2
1Chamarajnagar Institute of Medical Sciences, Karnataka, India. 2Yenepoya Medical College, Karnataka, India
*Corresponding author: K. T. Athulya Krishna Kumar; *Email: athunambiar156@gmail.com
Received: 15 Dec 2024, Revised and Accepted: 24 Feb 2025
ABSTRACT
Objective: Abnormal uterine bleeding (AUB) can be defined as any bleeding that varies from the duration, frequency and amount of blood flow in a normal menstrual cycle. In India, the prevalence of AUB in India is reported to be 17.9% with greater than one third of patients presenting with to the outpatient department with AUB. The endometrium is a hormone-sensitive and dynamic tissue and its histomorphological study along with clinical correlation is important in deciphering causes of AUB; to provide comprehensive patient care. This study aimed to analyze the histopathology of the endometrium and evaluate causes of abnormal uterine bleeding in conjunction with clinical findings.
Methods: This was a prospective study performed over a period of 2 y (2016-2018). The study comprised of 60 participants who came to the gynecology OPD with complaints of AUB. The relevant clinical information obtained and tabulated. Endometrial samples and hysterectomy specimens received in our pathology department were histopathologically analyzed and diagnosed.
Results: The age of the patients diagnosed ranged from 25-70 y and was maximally seen between 40-50 y (n=25, 41.67%). The most common clinical complaint was heavy menstrual bleeding (menorrhagia) (n=40, 66.67%). Histopathologically, endometrial hyperplasia was the most common pattern observed (n=20, 33.33%). In cases of anovulatory endometrium (n=18, 30%) the most common pattern was disordered proliferative endometrium (n=10, 16.67%).10 cases of endometrioid endometrial adenocarcinoma (16.67%).
Conclusion: Histopathological study of the endometrium, coupled with adequate clinical history is of utmost importance in eliciting the cause of AUB, with subsequent patient management.
Keywords: Abnormal uterine bleeding, Endometrium, Endometrial hyperplasia, Histopathology, Endometrial sampling
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i2.6079 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
The normal menstrual cycle duration varies from 21-35 d with the period of menstrual blood flow being 2-7 d. Average amount of blood lost during each menstrual flow is 20-80 ml [1, 2].
Any digression from the normal pattern of the menstrual cycle is deemed as abnormal. In postmenopausal women, any vaginal bleeding is considered as abnormal [2-4]. Abnormal uterine bleeding (AUB) can be defined as any bleeding that varies from the duration, frequency and amount of blood flow in a normal menstrual cycle [5] AUB may be divided into two groups, the first due to organic causes and the second in the absence of any organic causes, also termed as Dysfunctional uterine bleeding [2, 6].
Healthcare bodies such as American College of Obstetricians and Gynecologists (ACOG) and The International Federation of Gynecology and Obstetrics (FIGO) have suggested systematic nomenclature, which is the PALM-COEIN acronym, [Polyp, Adenomyosis, Leiomyoma, Malignancy, and Hyperplasia, Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic, and Not yet classified] to describe various causes of abnormal menses [7, 8].
The PALM-COEIN acronym is based on aetiopathogenesis wherein PALM describes organic causes of AUB and COIEN entails its non organic causes. Another term used frequently in this context is Heavy Menstrual Bleeding (HMB; menorrhagia) which is not synonymous with AUB, and is defined as excessive blood loss during menstrual cycle that interferes with a woman’s emotional, social and physical quality of life [7, 8]. A comprehensive assessment of the history and clinical examination in conjunction with blood tests, radiology and histopathology are needed to investigate causes of AUB [7].
In India, the prevalence of AUB in India is reported to be 17.9% [7, 8] Studies have reported that the prevalence varies between 10-30% according to different regions [9-11]. Greater than one third of patients present with to the outpatient department (OPD) with AUB. Uniform clinical practices are required for the management of this common ailment in a large and diverse population such as ours [7, 8].
The endometrium is a hormone-sensitive and dynamic, and tissue which constantly undergoes cyclical changes during reproductive life. The histomorphological study of the endometrium and screening for any pathology is a cornerstone to evaluate AUB.
Various factors such as age, menstrual cycle phase, parity, and utilization of exogenous hormones play an important role [12].
The goal of management is to adequately identify patients who have the risk of developing carcinoma and to diagnose potentially pre cancerous lesions such as endometrial hyperplasia with atypia by histopathological examination, which remains the gold standard [7, 8].
The present study was performed to analyze the histopathology of the endometrium and evaluate the causes of abnormal uterine bleeding in conjunction with clinical findings.
MATERIALS AND METHODS
This was a prospective study performed over a period of 2 y (2016-2018). The study comprised of 60 participants who came to the gynecology OPD with complaints of AUB.
The relevant clinical information, laboratory data and radiological findings was obtained and tabulated. Samples of endometrial biopsy, curettage and hysterectomy specimens received in the Department of Pathology at our tertiary care centre were processed and subsequently analyzed.
The specimens were fixed in ten percent formalin. The paraffin embedded 3-5 microns sections stained with Hemotoxylin and eosin (H and E) were studied for histopathological features under light microscopy. Cases with a clinical diagnosis of endometrial causes of AUB were included in this study. Women with other uterine pathology, cervical, vaginal and/or haemostatic pathology were excluded from this study. Institutional ethical committee clearance and patients informed consent was obtained.
RESULTS
The age of the patients diagnosed ranged from 25-70 y and was maximally seen between 40-50 y (n=25, 41.67%). It was more common in parous women (n=45, 75%) than in nulliparous women (n=15, 25%) (fig. 1). The most common clinical complaint was heavy menstrual bleeding (menorrhagia) (n=40, 66.67%), followed by heavy and prolonged bleeding (polymenorrhagia) (n=8, 13.33%), postmenopausal bleeding (n=10, 16.67%) and intermenstrual bleeding (metrorrhagia) (n=2, 3.33%) (table 1)
On histopathological examination (table 2), endometrial hyperplasia was the most common pattern observed (n=20, 33.33%). Endometrial hyperplasia cases comprised of 15cases of hyperplasia without atypia (fig. 2) and 5 cases of atypical hyperplasia (fig. 3). All cases of endometrial hyperplasia were noted in the 4th and 5th decades.
In cases of anovulatory endometrium (n=18, 30%) the most common pattern was disordered proliferative endometrium (n=10) followed by proliferative endometrium (n=8)
10 cases of endometrioid endometrial adenocarcinoma (fig. 4) were diagnosed out of which 5 cases belonged to FIGO grade 1, 3 cases were of FIGO Grade 2 and 2 cases were FIGO grade 3. All carcinoma cases were seen between ages of 50-70.
There were 8 cases (13.33%) diagnosed with endometrial polyp (fig. 5) and 4 cases (6.67%) of secretory endometrium.
Table 1: Clinical presentation of AUB
| Pattern of bleeding | Age group | Total N (%) | ||||
| 20-30 y | 30-40 y | 40-50 y | 50-60 y | 60-70 y | ||
| Menorrhagia | 05 (8.33%) | 11 (18.33%) | 24 (40%) | - | - | 66.67% |
| Polymenorrhagia | 01 (1.67%) | 02 (3.33%) | 01 (1.67%) | 04 (6.67%) | - | 08 (13.33%) |
| Metrorrhagia | 01 (1.67%) | 01 (1.67%) | - | - | - | 02 (3.33%) |
| Post menopausal bleeding | - | - | - | 06 (10%) | 04 (6.67%) | 10 (16.67%) |
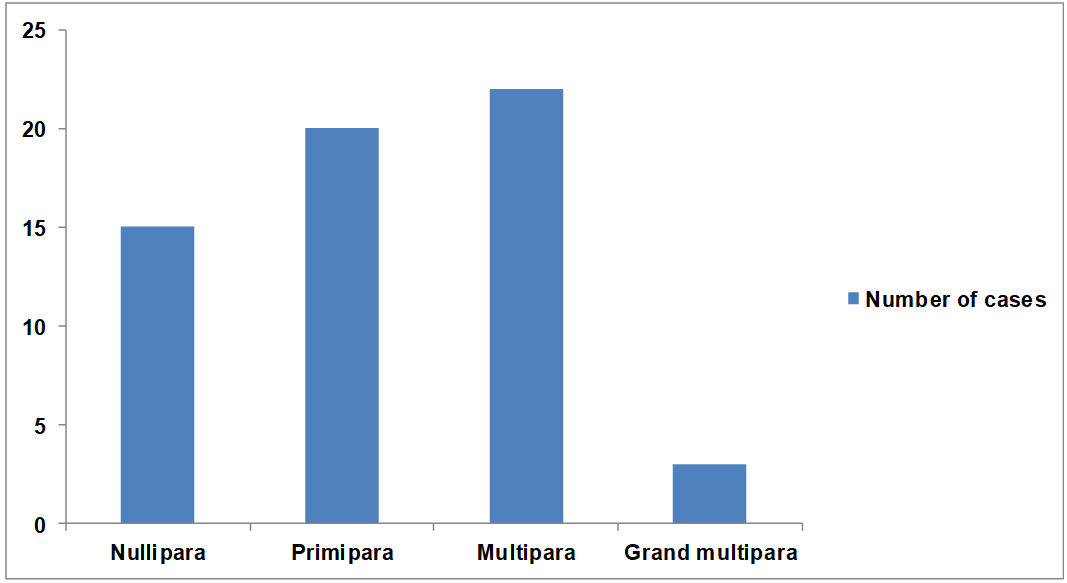
Fig. 1: Distribution of women according to parity
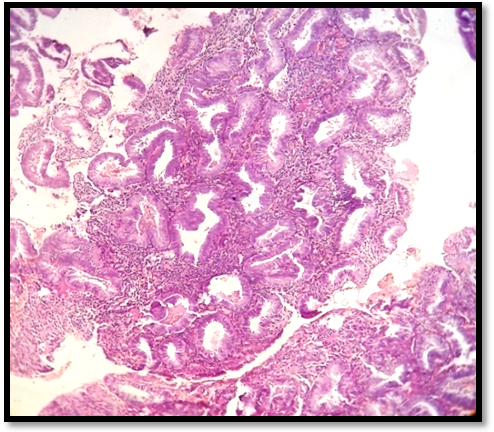
Fig. 2: Photomicrograph showing endometrial glands in hyperplasia without atypia (H and E, 10x)
Table 2: Histopathological findings in endometrium and its distribution with regard to age group
| Histopathology | Age group | Total N (%) | ||||
| 20-30 y | 30-40 y | 40-50 y | 50-60 y | 60-70 y | ||
| Disordered proliferative | 01 (1.67%) | 07 (11.67%) | 02 (3.33%) | - | - | 10 (16.67%) |
| Proliferative endometrium | 04 (6.67%) | 03 (5%) | 01 (1.67%) | - | - | 8 (13.33%) |
| Secretory endometrium | - | 03 (5%) | 01 (1.67%) | - | - | 4 (6.67%) |
| Endometrial polyp | 02 (3.33%) | 01 (1.67%) | 05 (8.33%) | - | - | 8 (13.33%) |
| Hyperplasia without atypia | - | - | 13 (21.67%) | 02 (3.33%) | - | 15 (25%) |
| Atypical endometrial hyperplasia | - | - | 03 (5%) | 02 (3.33%) | - | 5 (8.33%) |
| Endometrioid adenocarcinoma | - | - | - | 06 (10%) | 04 (6.67%) | 10 (16.67%) |
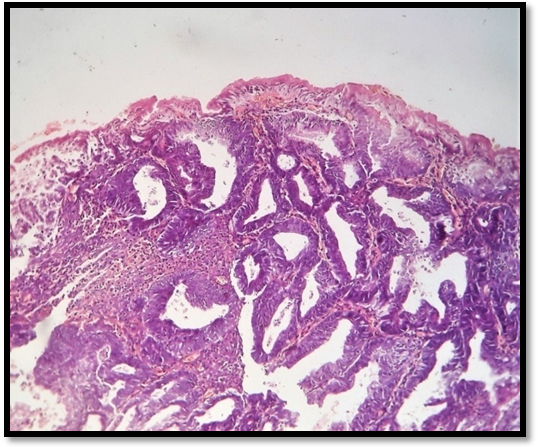
Fig. 3: Photomicrograph showing endometrial glands in hyperplasia with atypia (H and E, 10x)
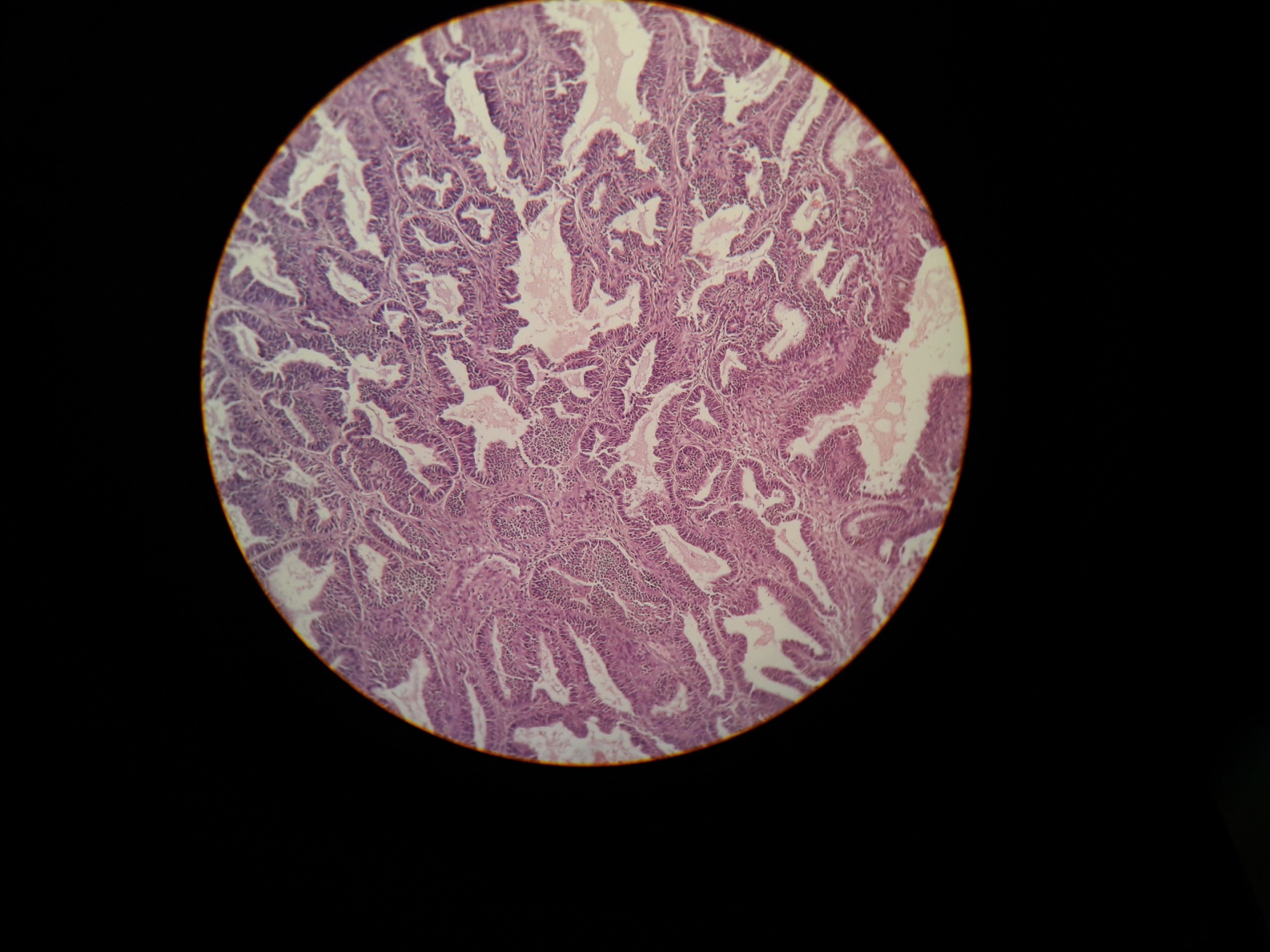
Fig. 4: Photomicrograph of well differentiated endometrial carcinoma (H and E, 10x)
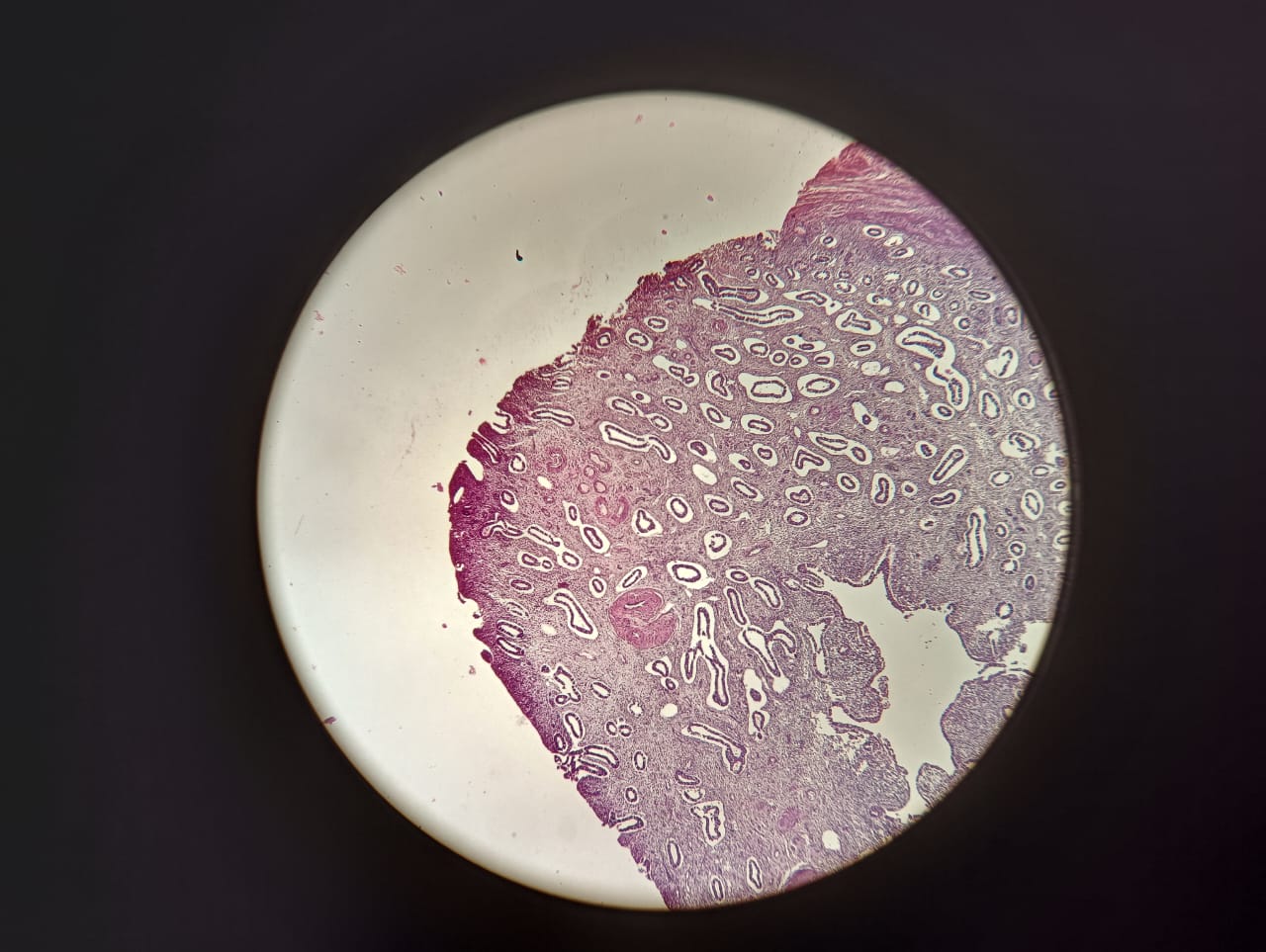
Fig. 5: Photomicrograph of endometrial polyp. (HandE, 4x)
DISCUSSION
AUB is a common gynecological complaint accounting for 20% OPD visits and almost 25% of gynecological surgeries [13]. The three-pronged approach combining history collection, imaging modalities and histopathological analysis of endometrial samples are of utmost importance in patient care. This is vital, especially in cases where there is a serious underlying condition in the endometrium, wherein major surgical procedures and aggressive treatment may be necessary [5].
The most common age group in our study was 40-50 y (41.67%). Similar findings were reported by Muzaffar et al. [14] and Thanyapa W [15], wherein most cases of AUB most of the abnormal uterine bleeding occurred between ages of 40-50 y.
Muzaffar M et al. [14] also reported menorrhagia as the commonest presenting symptom, accounting for 51.9% cases. Bhosle A et al. showed menorrhagia as the major clinical complaint in women having abnormal uterine bleeding. [16] This was in conjunction with the findings of our study, where there was a striking majority of cases presenting with menorrhagia (heavy menstrual bleeding (66.67%). There were 10 cases (16.67%) in our study who presented with post-menopausal bleeding, which was comparable to study done by Katuwal N (N=9, 7.5%) [2].
In an anovulatory cycle there is excess estrogen stimulation coupled with proliferation, which may lead to endometrial hyperplasia and if unchecked, endometrial carcinoma [2, 3].
In the present study, endometrial hyperplasia (33.33%) was the most common pattern seen. In this maximum case comprised of hyperplasia without atypical (75%). Several previous studies corroborated with this finding. Shah R et al. reported a majority of endometrial hyperplasia cases in their study (42.9%) [17] Bindhuja J et al. reported the most common pattern to be simple cystic endometrial hyperplasia (28%) [5].
The second most frequent pattern noted in our study was anovulatory endometirum (30%) comprising of disordered proliferative endometrium and proliferative endometrium. Sarwar Aet al. [18] had similar findings in their study (24% cases)
Endometrial carcinoma is an important differential diagnosis in women of both peri and post-menopausal age group. We reported 10 cases of endometrial adenocarcinoma (16.67%) where post-menopausal bleeding was the primary clinical complaint. Bindhuja J et al. [5] and Sarwar A [18] reported similar findings in their respective studies.
CONCLUSION
In the present study, endometrial hyperplasia was found to be the most common cause of AUB, followed by anovulatory endometrial pattern. Menorrhagia was the commonest clinical finding. Abnormal uterine bleeding needs thorough investigation to identify the underlying cause, along with prompt intervention to avoid complications. Correlation of clinical data and histopathologic features are vital for diagnosis and further patient management.
ACKNOWLEDGEMENT
None
FUDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICTS OF INTERESTS
Declared none
REFERENCES
Algotar KM, Nalawade A. Physiology of menstruation. In: Purandare CN, editor. Dysfunctional uterine bleeding an update. New Delhi: Jaypee. Jaypee Brothers Medical Publishers (P) Ltd; 2004. p. 1-15. doi: 10.5005/jp/books/10246_1.
Katuwal N, Gurung G, Rana A, Jha A. A clinicopathological study of dysfunctional uterine bleeding. J Pathol Nep. 2014;4(8):635-8. doi: 10.3126/jpn.v4i8.11500.
Kumar P, Malhotra N, Editors. Menopause. Jeffcoate’s principal of gynecology. New Delhi: Jaypee; 2008. p. 862-4.
Rock J, Jones H, Editors. Normal and abnormal uterine bleeding. Te Linde’s operative gynecology. Philadelphia: Lippincott Williams & Wilkins; 2009. p. 585-92.
Bindhuja J. Histopathologic study of endometrium in cases of abnormal uterine bleeding. J Pathol Nep. 2023;13(1):1983-6. doi: 10.3126/jpn.v13i1.40891.
Davey DA. Dysfunctional uterine bleeding. In: Whitfield CR, editor. Dewhurst’s Textbook of obstetrics and gynecology for postgraduates. Oxford: Blackwell Publishing Science; 1995. p. 624-45.
Vaidya R, Vinayachandran S, Sumangala D, Prejisha B, Lekshminath G, Sily S. Prevalence of abnormal uterine bleeding and its associated risk factors in women of perimenopausal age group: a retrospective study. J Clin Diagn Res. 2022;16(12):QC09-13.
Munro MG, Critchley HO, Fraser IS. Committee the two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Intl J Gynecology & Obste. 2018;143(3):393-408. doi: 10.1002/ijgo.12666.
Sharma A, Dogra Y. Trends of AUB in tertiary centre of Shimla hills. J Mid Life Health. 2013;4(1):67-8. doi: 10.4103/0976-7800.109648, PMID 23833543.
Kazemijaliseh H, Ramezani Tehrani FR, Behboudi Gandevani S, Khalili D, Hosseinpanah F, Azizi F. A population-based study of the prevalence of abnormal uterine bleeding and its related factors among iranian reproductive age women: an updated data. Arch Iran Med. 2017;20(9):558-63. PMID 29048917.
Kotagasti T. Prevalence of different menstrual irregularities in women with abnormal uterine bleeding (AUB): an observational study. Int J Curr Res. 2015;7(10):66-70.
Jairajpuri ZS, Rama S, Jetky S. Cal uterine bleeding: histopathological audit of endometrium: a study of 638 cases. Al Ameen J Med Sci Atypi. 2013;6:21-8.
Khare A, Bansal R, Sharma SP, Elhence N, Makkar Y, Tyagi Y. Morphological spectrum of endometrium in patients presenting with dysfunctional uterine bleeding. Peoples J Sci Res. 2012;5:13-6.
Khan IA. Nocturnal enuresis. J Pak Med Assoc. 2005;55(1):1. PMID 15816685.
Thanyapa W. Histopathological result of fractional curettage in Satuk Hospital. Siriraj Med J. 2010;25:93-100.
Bhosle A, Fonseca M. Evaluation and histopathological correlation of abnormal uterine bleeding in perimenopausal women. Bombay Hosp J. 2010;52:69-72.
Shah R, Dayal A, Kothari S, Patel S, Dalal B. Histopathological interpretation of endometrium in abnormal uterine bleeding. Int J Med Sci Public Health. 2014;3(4):452-6. doi: 10.5455/ijmsph.2014.120220142.
Sarwar A, Haque A. Types and frequencies of pathologies in endometrial curettings of abnormal uterine bleeding. Int J Pathol. 2005;3:65-70.