
Int J Curr Pharm Res, Vol 17, Issue 2, 93-95Case Study
A RARE CASE OF TESTICULAR MIXED GERM CELL TUMOUR WITH POLYEMBRYOMA AND MATURE TERATOMA COMPONENTS
PRAGNYA PARAMITA MISHRA1*, PREMANAND PANDA2
1Department of Pathology, Hi-tech MCH, Rourkela, Odisha, India. 2Department of Radiology, JP Hospital and Research Centre, Rourkela, Odisha, India
*Corresponding author: Pragnya Paramita Mishra; *Email: pparamita1982@gmail.com
Received: 16 Dec 2024, Revised and Accepted: 25 Feb 2025
ABSTRACT
Polyembryoma of the testis is an extremely rare and distinct form of mixed germ cell tumor with recapitulation of embryoid bodies where yolk sac, embryonal, and teratoma components can be found. Our case is a 27-year-old male presented with a painless mass in the left scrotum, which was progressively increasing over the last 3 mo. Serum Alpha-fetoprotein and beta HCG were marginally elevated. Fine needle aspiration cytology (FNAC) was suggestive of a non-seminomatous germ cell tumor of the testis. Histopathology of the orchidectomy specimen revealed a predominant polyembryoma with an immature teratoma component with a diagnosis of mixed germ cell tumor. Immunohistochemistry confirmed the diagnosis, and the patient was on adjuvant chemotherapy. We are reporting the case because of extreme rarity.
Keywords: Diagnosis, Testis, Mixed germ cell tumor, Mature teratoma, Polyembryoma
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i2.6085 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Testicular cancer is a rare neoplasm, and about 1 of every 250 males will develop testicular cancer at some point during their lifetime. It accounts for up to 10 percent of all malignant diseases that affect the male genitourinary system and make up about 2 percent of all malignant tumors in men. More significantly, testis tumors rank third in terms of causes of mortality for males in the 20–40 age range and are the most prevalent malignant disease in this age group [1].
Testicular tumors are broadly divided into germ cell tumors and sex cord-stromal tumors; the former constitute about 95% of all. Again, germ cell tumors are divided into seminomatous and nonseminomatous germ cell tumor (NSGCT) types. Non-seminomatous tumors may be composed of undifferentiated cells that resemble embryonic stem cells, as in embryonal carcinoma but can differentiate into various lineages, generating yolk sac tumors, choriocarcinomas, and teratomas [2]. However, mixed germ cell tumors, which comprise 32% to 60% of all germ cell tumors, are significantly more common in young males than any of the pure histologic types and are characterized by the presence of multiple germ cell components. The composition of these tumors varies [3]. The polyembryoma is a distinctive, very rare, well-organized form of mixed germ cell tumor consisting of embryonal carcinoma and yolk sac tumor [4].
RESULTS
A 27-year-old male has presented with a painless mass in the left scrotum, which was progressively increasing over the last 3 mo. Other general examination was within normal limits. Local Examination showed a mass in the left scrotum. Routine blood investigation was performed, which was within normal limits. A pelvic ultrasound showed a left testicular mass measuring 6.5 x 5.5 x 4.4 cm with calcifications and solid-cystic areas, suspicious for malignancy. The vasculature was normal. The A chest X-ray and CT scan of the abdomen and pelvis were normal. Tumor markers were sent, which showed serum alpha-fetoprotein was 560 IU/l, and beta HCG was marginally elevated. Based on this, the presence of a mixed germ cell tumor was suspected, and the patient was subjected to FNAC, which was suggestive of a germ cell tumor of the testis (non-seminomatous). (fig. 1).

Fig. 1: Microphotograph showing malignant cells in clusters in 40x
The patient underwent a left orchidectomy. Grossly, the testis showed a well-circumscribed, homogenous, capsulated tumor (fig. 2). Measuring 6.0 x 5.0 x 4.2 cm with a variegated cut surface. Areas of hemorrhage and necrosis not seen.

Fig. 2: Gross picture showing a well-circumscribed, homogenous, capsulated tumor
In histopathology, a diagnosis of mixed germ cell tumor was offered with predominant polyembryoma (75%) (fig. 4 and 5)and immature teratoma (25%) (fig. 3) components. The tumor was limited to one testis without any capsular invasion, lymphovascular invasion, or pelvic lymphadenopathy. Immunohistochemistry (fig. 6) confirmed the diagnosis, and the patient was on adjuvant chemotherapy. The patient is under regular follow-up.
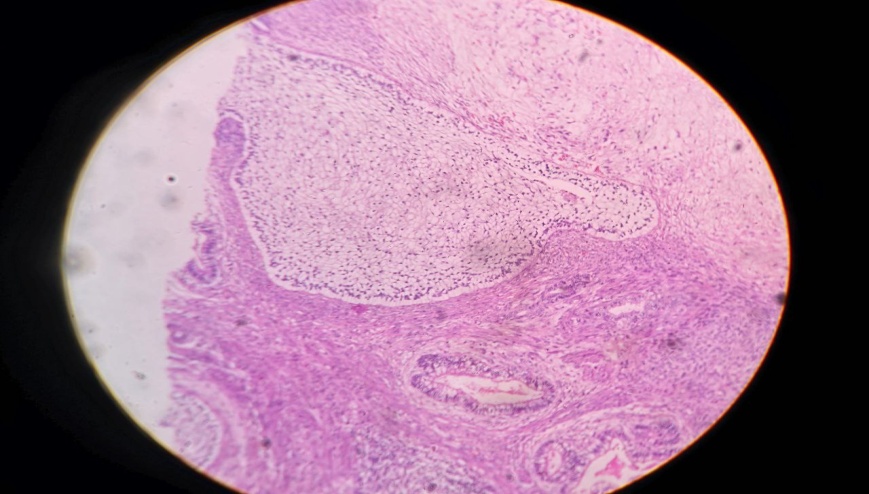
Fig. 3: Microphotograph showing teratoma component
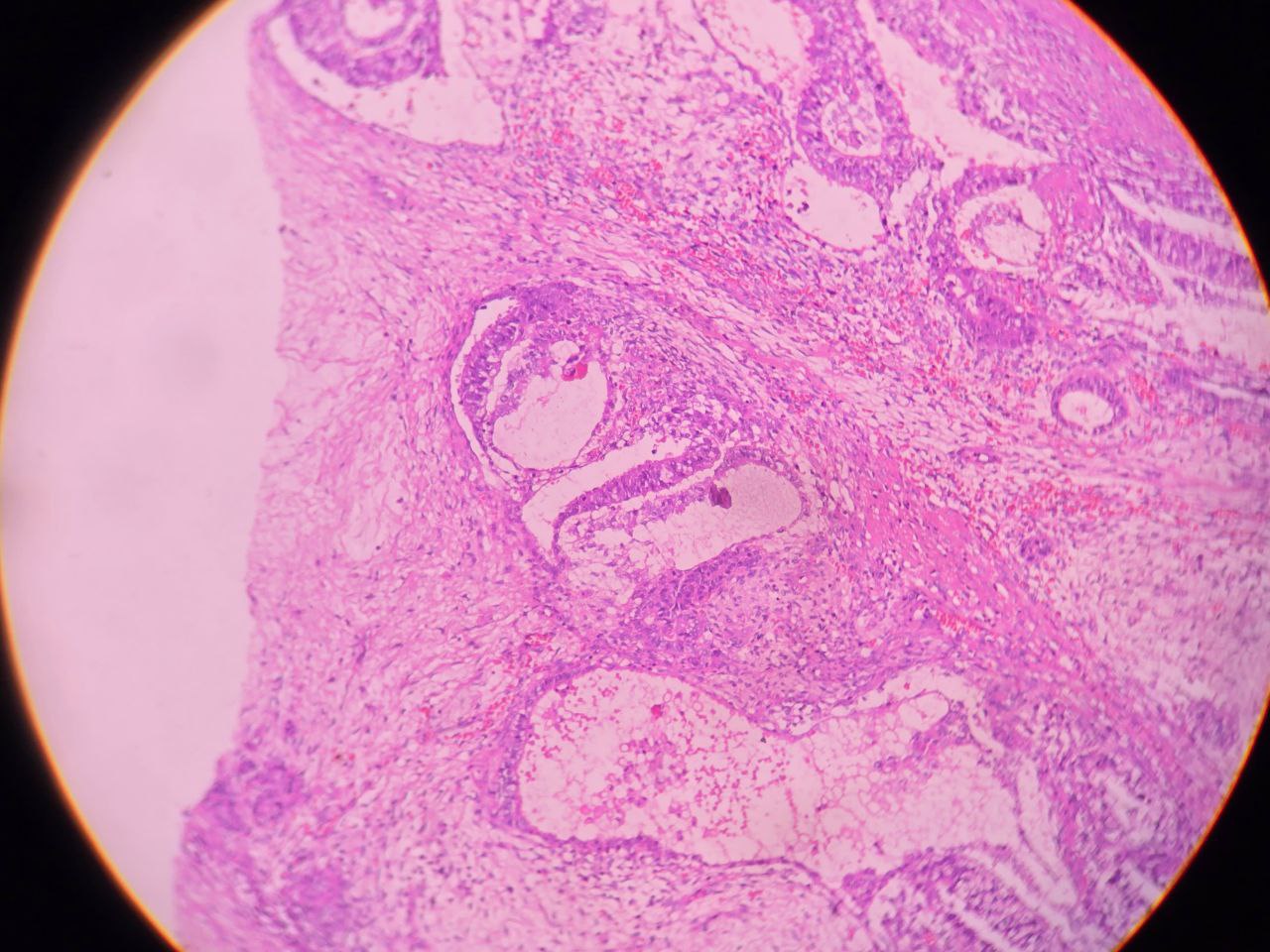
Fig. 4: Microphotograph showing polyembryoma component

Fig. 5: Microphotograph showing polyembryoma component
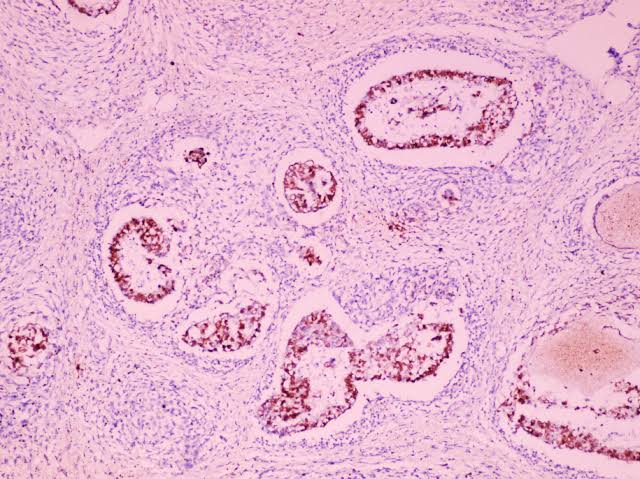
Fig. 6: Microphotograph showing AFP IHC confirming yolksac component
DISCUSSION
Testicular cancer is a rare neoplasm, and Polyembryoma is an extremely rare type of mixed germ cell malignancy. Identification of polyembryoma by the pathologist may have several practical points in addition to mere academic interest prompted by the remarkable morphology: explanation of an elevated AFP level and awareness of the Morphology will aid identification at extragonadal primary and metastatic sites. Serial measurements of these tumor markers have been useful in the diagnosis, monitoring response to treatment, and follow-up during remission to detect early recurrence.
In the previous cases available in the search engine, the cases ranged from 28 to 60 years, with three being in their 20s, three in their early to mid-40s, and one being a 60 y old with a history of Hodgkin’s lymphoma. In the case with gynecomastia, the the patient had a minor choriocarcinoma component.
The embryoid body-the unit of polyembryoma is a typically spherical to oval development with a thin, wispy layer of yolk sac epithelium underneath a central germ disk made of embryonal carcinoma-type epithelium. There are cavities that mimic the amniotic cavity above the germ. disc and, occasionally, the yolk sac vesicle below. Embryoid bodies are encircled by a thick cuff of edematous to myxoid stroma; lobulation can occasionally be a noticeable low-power view.
CONCLUSION
Testicular Mixed germ cell tumors are quite uncommon and often affect young males. Another An uncommon form of MGCT is polyembryoma. Because of its biological behavior, clinical care, and prognosis vary depending on its various histological components, it remains a diagnostically problematic issue. As a result, precise Pathology diagnosis is crucial, and immunohistochemistry is crucial for both. diagnosing and excluding different aspects of testicular MGCT.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCESReferences
Coleman MP, Esteve J, Damiecki P, Arslan A, Renard H. Trends in cancer incidence and mortality. IARC Sci Publ. 1993;(121):1-806. doi: 10.3109/9780415874984-2, PMID 8258476.
Kumar V, Abbas AK, Fausto N, Aster J. The male Ge nital tract. In: Robbins and Cotran pathologic. Basis of disease. 8th ed. Saunders, Elsevier Incorporated; 2010. p. 987-93.
Stamatiou K, Papadopoulos P, Perlepes G, Galariotis N, Olympitis M, Moschouris H. Mixed germ cell tumor of the testicle with rhabdomyosarcomatous component: a case report. Cases J. 2009 Dec 10;2:9299.
Ulbright TM. Germ cell neoplasms of the testis. Am J Surg Pathol. 1993;17(11):1075-91. doi: 10.1097/00000478-199311000-00001, PMID 8214253.