
Int J Curr Pharm Res, Vol 17, Issue 4, 88-93Original Article
WORMIAN BONES IN THE HUMAN SKULL: ANATOMICAL DISTRIBUTION, SHAPE PATTERNS, AND ASSOCIATION WITH CRANIAL SUTURE LENGTHS
ASHOK PAL GOBIND¹, VIDYA R. PILLAI², RITURAJ MAJUMDER³, ARBIND KUMAR CHOUDHARY⁴*
1,3Department of Anatomy, Andaman and Nicobar Islands Institute of Medical Sciences (ANIIMS), Sri Vijaya Puram, Andaman and Nicobar Islands, India. 2Department of Anatomy, A. J. Institute of Medical Sciences and Research Centre, Kuntikana, NH-66, Mangalore-575004, Karnataka, India. 4Department of Pharmacology, Government Erode Medical College and Hospital, Erode, Tamil Nadu-638002, India
*Corresponding author: Arbind Kumar Choudhary; *Email: arbindkch@gmail.com
Received: 15 Apr 2025, Revised and Accepted: 10 Jun 2025
ABSTRACT
Objective: To investigate the prevalence, anatomical distribution, and morphological characteristics of Wormian bones in adult human skulls, and to assess their association with the lengths of major cranial sutures.
Methods: A total of 125 fully ossified adult skulls were examined from osteological archives at ANIIMS (Port Blair) and AJIMS and RC (Mangaluru). Wormian bones were identified across predefined cranial suture sites. Their shape and edge morphology were categorized, and the lengths of the sagittal, coronal, and lambdoid sutures were measured using standardized osteometric techniques. Group comparisons were performed using independent t-tests.
Results: Wormian bones were present in 48.8% of specimens. The lambdoid suture was the most frequently involved site, followed by the lambda and sagittal sutures. Quadrangular ossicles were the predominant morphological type. Comparative analysis revealed no statistically significant differences in mean cranial suture lengths between skulls with and without Wormian bones (p>0.05).
Conclusion: Wormian bones represent common anatomical variants in the examined population, with a predilection for the posterior cranial vault. Despite their morphologic variability, they do not significantly influence the linear dimensions of major cranial sutures. Recognizing their typical features and locations is essential for accurate radiological assessment and anthropological documentation.
Keywords: Wormian bones, Cranial sutures, Sutural ossicles, Anatomical variation, Lambdoid suture, Skull morphometry, Forensic anthropology
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i4.7020 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Wormian bones, also known as sutural or intra-sutural bones, are accessory ossicles that arise within the cranial sutures due to additional centers of ossification during calvarial development. These bones are typically small, irregular in shape, and most frequently located along the lambdoid suture. However, they may also occur in the sagittal, coronal, asterion, pterion, and at the lambda-the junction of the sagittal and lambdoid sutures [1, 2]. Though often regarded as normal anatomical variants, Wormian bones possess substantial clinical, anthropological, and developmental significance.
Embryologically, these bones result from supernumerary ossification centers that develop during intramembranous ossification of the skull vault. The complexity of suture patterns, particularly in the posterior cranium, and the prolonged ossification timeline of sutures such as the lambdoid, contribute to their formation [3, 4]. Mechanical factors, including molding forces during parturition and postnatal cranial growth, are also believed to play a contributory role [5]. Morphologically, Wormian bones may exhibit diverse shapes-quadrangular, triangular, or irregular-and possess either smooth (serpiginous) or jagged margins, reflecting the heterogeneity in ossification dynamics.
Clinically, the recognition of Wormian bones is crucial. On radiographic imaging, especially in infants and young children, they can mimic skull fractures or suture diastasis, potentially leading to misinterpretation and unnecessary intervention [6, 7]. Moreover, an increased number of Wormian bones, particularly in atypical locations or with abnormal morphology, is frequently reported in association with skeletal dysplasias such as osteogenesis imperfecta, cleidocranial dysostosis, rickets, hypothyroidism, and craniosynostosis syndromes [7, 8]. Their identification can therefore serve as a valuable diagnostic clue in both pediatric and genetic evaluations.
From a forensic and anthropological standpoint, the presence, number, and anatomical distribution of Wormian bones provide insights into population-based cranial variability, ancestry, and phylogenetic trends [9, 10]. Their prevalence has been shown to vary considerably across ethnic groups, with higher incidences documented in Asian, South American, and certain indigenous populations [11, 12]. However, despite this relevance, systematic morphometric data regarding Wormian bones in Indian populations-particularly from the South Indian and Andaman regions-remain sparse.
Another aspect that warrants attention is the potential relationship between the presence of Wormian bones and cranial suture lengths. While some hypotheses suggest that longer or more tortuous sutures may be more susceptible to accessory ossicle formation, evidence remains inconclusive. Few studies have quantitatively explored whether a morphometric correlation exists between the presence of Wormian bones and the linear dimensions of major cranial sutures such as the sagittal, coronal, and lambdoid [13, 14].
In this context, the present study was designed with two primary objectives: (1) to determine the prevalence, anatomical distribution, and morphological characteristics of Wormian bones in adult human skulls from two distinct Indian coastal populations; and (2) to evaluate whether a statistically significant association exists between the presence of these bones and the lengths of major cranial sutures. This investigation seeks to contribute novel anatomical insights while addressing an existing gap in regional morphometric data.
MATERIALS AND METHODS
Study design and ethical approval
This was a descriptive, cross-sectional osteological study conducted across two academic centers: the Department of Anatomy at Andaman and Nicobar Islands Institute of Medical Sciences (ANIIMS), Port Blair, and the A. J. Institute of Medical Sciences and Research Centre (AJIMS and RC), Mangaluru. The study protocol was reviewed and approved by the Institutional Ethics Committee of ANIIMS (Approval No. ANIIMS/IEC/2022-23/26), in accordance with the Indian Council of Medical Research (ICMR) guidelines for the ethical use of human skeletal material.
Sample selection
A total of 125 adult, fully ossified human skulls were analyzed. These specimens were part of the teaching osteology collections at the participating institutions. The sex and age of the skulls were unknown. Inclusion criteria comprised skulls with complete cranial vaults and clearly visible cranial sutures. Skulls showing signs of trauma, pathology, congenital deformities, or post-surgical alterations were excluded to ensure morphometric validity.
Examination protocol
Each skull was systematically examined for the presence of Wormian bones at key cranial suture sites. The predefined anatomical sites included the lambdoid suture, sagittal suture, coronal suture, lambda (the junction of sagittal and lambdoid sutures), pterion, asterion, parietomastoid, parietosquamous, and occipitomastoid regions. Observations were conducted independently by two anatomists with experience in cranial osteology. In instances of observational discrepancy, a joint re-evaluation was undertaken to reach consensus.
Morphological characterization of wormian bones
Wormian bones identified were characterized based on their shape-categorized as quadrangular, triangular, or irregular-and by their marginal morphology, classified as either serpiginous (smoothly undulating) or irregular (jagged or fragmented). Digital photography was used to document representative specimens at each anatomical site.
Cranial suture length measurement
To assess morphometric correlations, linear measurements of three major cranial sutures-sagittal, coronal, and lambdoid-were recorded.
Sagittal suture length was measured from bregma to lambda.
Coronal suture length was recorded from bregma to the right and left pterion, with the average used for analysis.
Lambdoid suture length was measured from lambda to the right and left asterion, again averaged for consistency.
Measurements were performed using a non-stretchable flexible tape (precision 0.01 cm) and verified with Vernier calipers for accuracy at anatomical endpoints.
Statistical analysis
Data were compiled in Microsoft Excel and analyzed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY). Descriptive statistics (mean, standard deviation, frequencies) were calculated for the prevalence and morphological features of Wormian bones. Independent samples t-tests were employed to compare mean suture lengths between skulls with Wormian bones (WB+) and those without (WB−). A p-value<0.05 was considered statistically significant.
RESULTS
Prevalence of wormian bones
Out of 125 adult crania evaluated, additional intrasutural ossicles-Wormian bones-were observed in 61 specimens, accounting for a prevalence of 48.8%. The remaining 64 skulls (51.2%) displayed no such accessory bones. Confidence intervals calculated for each group confirmed a nearly equal distribution between affected and unaffected skulls, as detailed in table 1.
Table 1: Incidence of wormian bones among 125 human skulls
| WB_Present | Number of skulls | Percentage (%) | 95% CI (%) | Description |
| Yes | 61 | 48.8% | 40.2 – 57.5% | Skulls exhibiting one or more Wormian bones |
| No | 64 | 51.2% | 42.5 – 59.8% | Skulls without any identifiable Wormian bones |
Note: Percentages are calculated from the total sample (n = 125). Confidence intervals were computed using the Wilson score method.
Anatomical distribution of wormian bones by suture
Among the 61 skulls with identified Wormian bones, the most frequently involved site was the lambdoid suture(16.39%), followed by the lambda (14.75%), sagittal (13.11%), and coronal (11.48%) sutures. Less frequent sites included the pterion, asterion, and parietomastoid (each 9.84%), parietosquamous (8.20%), and occipitomastoid (6.56%). These findings are summarized in table 2 and illustrated in fig. 1. Representative labeled anatomical images of Wormian bones at the lambda and lambdoid sutures are provided in fig. 2 and 3, respectively.
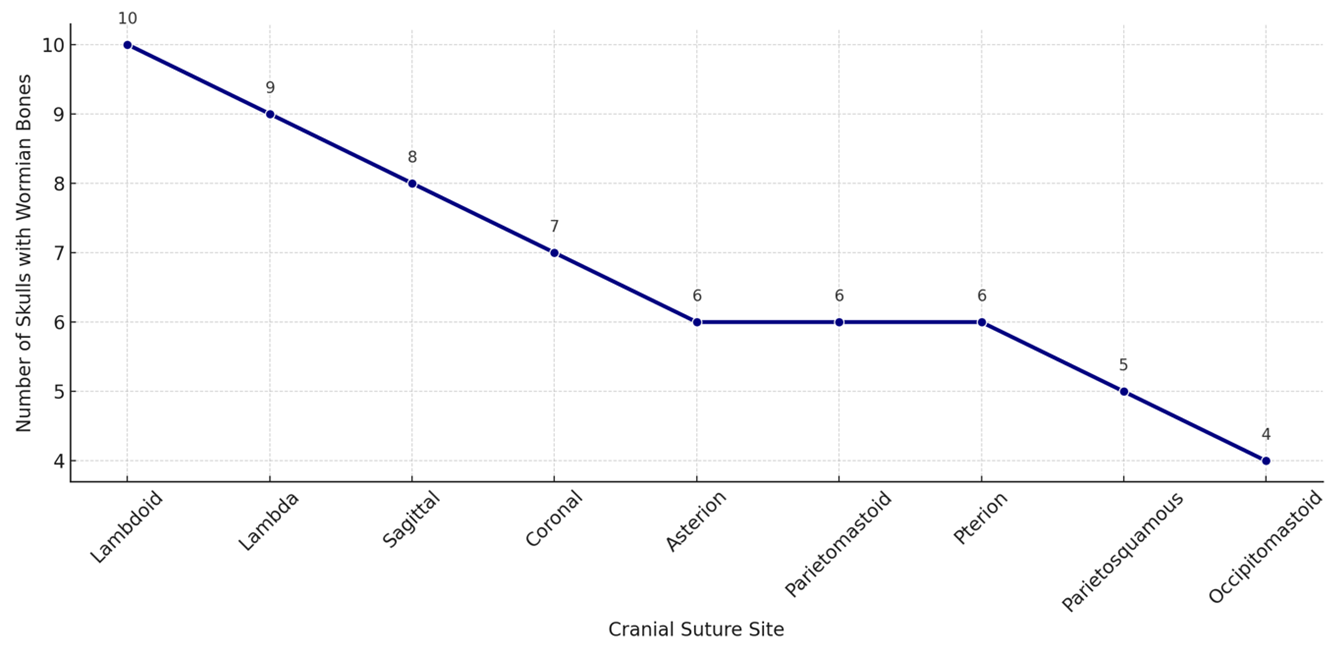
Fig. 1: Line graph showing frequency of wormian bones across cranial sutures
Table 2: Site-wise distribution of wormian bones (n = 61)
| Suture site | Number of skulls | Percentage (%) |
| Lambdoid | 10 | 16.39% |
| Lambda | 9 | 14.75% |
| Sagittal | 8 | 13.11% |
| Coronal | 7 | 11.48% |
| Asterion | 6 | 9.84% |
| Parietomastoid | 6 | 9.84% |
| Pterion | 6 | 9.84% |
| Parietosquamous | 5 | 8.20% |
| Occipitomastoid | 4 | 6.56% |
Percentages are based on the subset of skulls with wormian bones (n = 61). Some skulls exhibited multiple sites of involvement.
Fig. 1 line graph illustrating the anatomical distribution of Wormian bones across various cranial suture sites among 61 skulls. The lambdoid suture was the most frequently involved site (16.39%), followed by the lambda (14.75%) and sagittal (13.11%) sutures. Less commonly affected sutures included the coronal, asterion, parietomastoid, pterion, parietosquamous, and occipitomastoid regions. The graph demonstrates a descending trend in frequency from posterior to lateral and inferior cranial sutures.
Fig. 2 labeled photograph of a human skull illustrating a Wormian bone located at the lambda-the anatomical junction of the sagittal and lambdoid sutures. This Y-shaped confluence is a common site for accessory ossicles due to the complexity and late fusion of surrounding cranial bones.
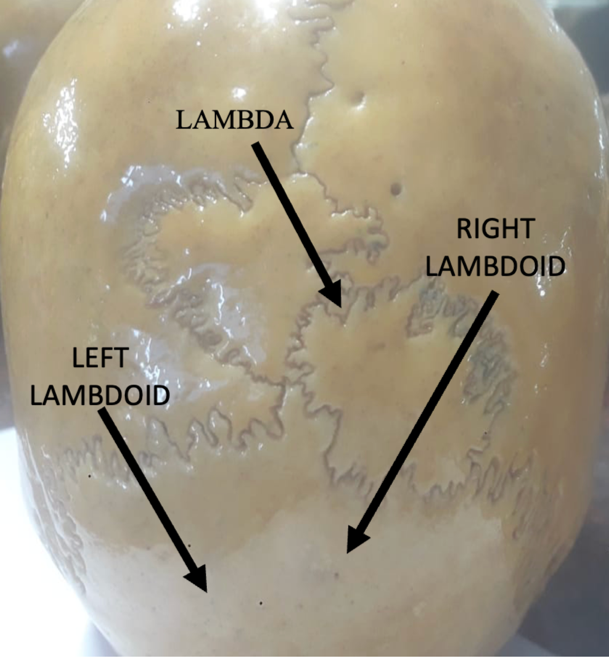
Fig. 2: Labeled image illustrating a wormian bone at the lambda (junction of sagittal and lambdoid sutures)
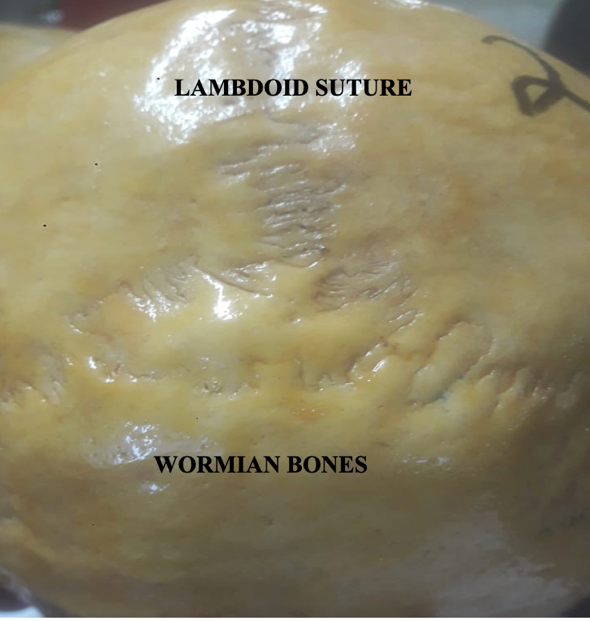
Fig. 3: Posterior skull view demonstrating wormian bones along the lambdoid suture
Fig. 3 Posterior view of a human skull demonstrating multiple Wormian bones situated along the lambdoid suture. The bones appear as small, irregular ossicles interposed between the parietal and occipital bones, a characteristic location due to the suture’s complex morphology and prolonged ossification period
Morphological characteristics of wormian bones
Wormian bones were classified based on their shape and edge morphology. The majority were quadrangular (47.76%), followed by irregular (38.81%), and triangular forms (13.43%). Regarding edge type, irregular margins were more commonly observed (59.7%) than serpigenous (smoothly undulating) borders (40.3%). The morphological distribution is provided in table 3, and shape proportions are depicted in fig. 4.
Table 3: Distribution of wormian bone shapes and edge types
| Type | Count | Percentage (%) | Category |
| Quadrangular | 43 | 47.76% | Shape |
| Irregular | 35 | 38.81% | Shape |
| Triangular | 12 | 13.43% | Shape |
| Irregular | 49 | 59.7% | Edge |
| Serpigenous | 33 | 40.3% | Edge |
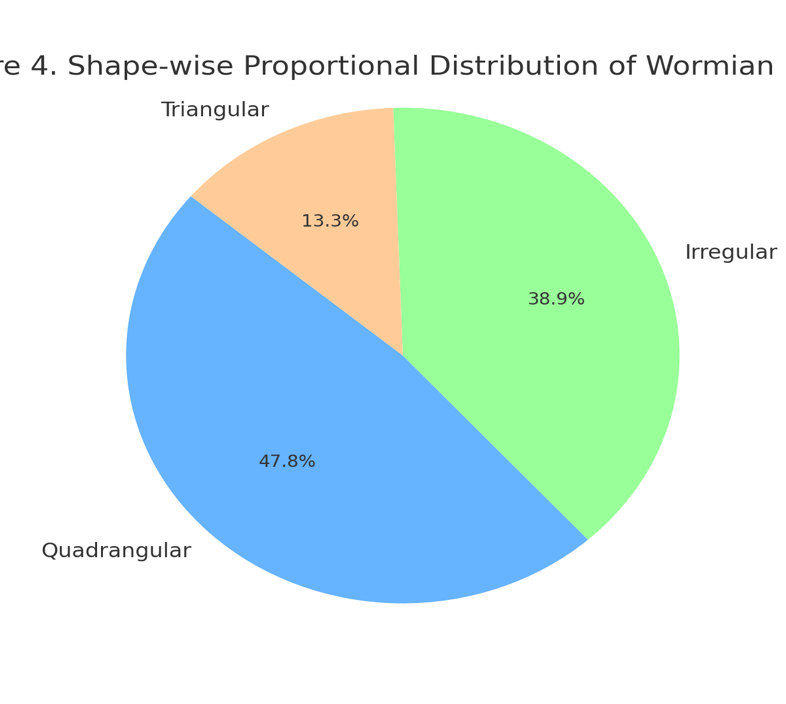
Fig. 4: Proportional distribution of wormian bones
Table 4: Comparison of suture lengths in skulls with and without wormian bones
| WB_present | Sagittal mean±SD (cm) | Sagittal (min–Max) | Coronal mean±SD (cm) | Coronal (min–Max) | Lambdoid mean±SD (cm) | Lambdoid (min–max) |
| No | 13.02±1.14 | 11.2 – 15.0 | 22.84±1.44 | 20.1 – 25.0 | 20.58±1.57 | 18.2 – 23.8 |
| Yes | 13.06±1.10 | 11.0 – 14.9 | 22.58±1.39 | 20.2 – 25.0 | 20.64±1.84 | 18.0 – 23.9 |
Note: Statistical analysis using independent t-tests revealed no significant differences between groups (p>0.05).
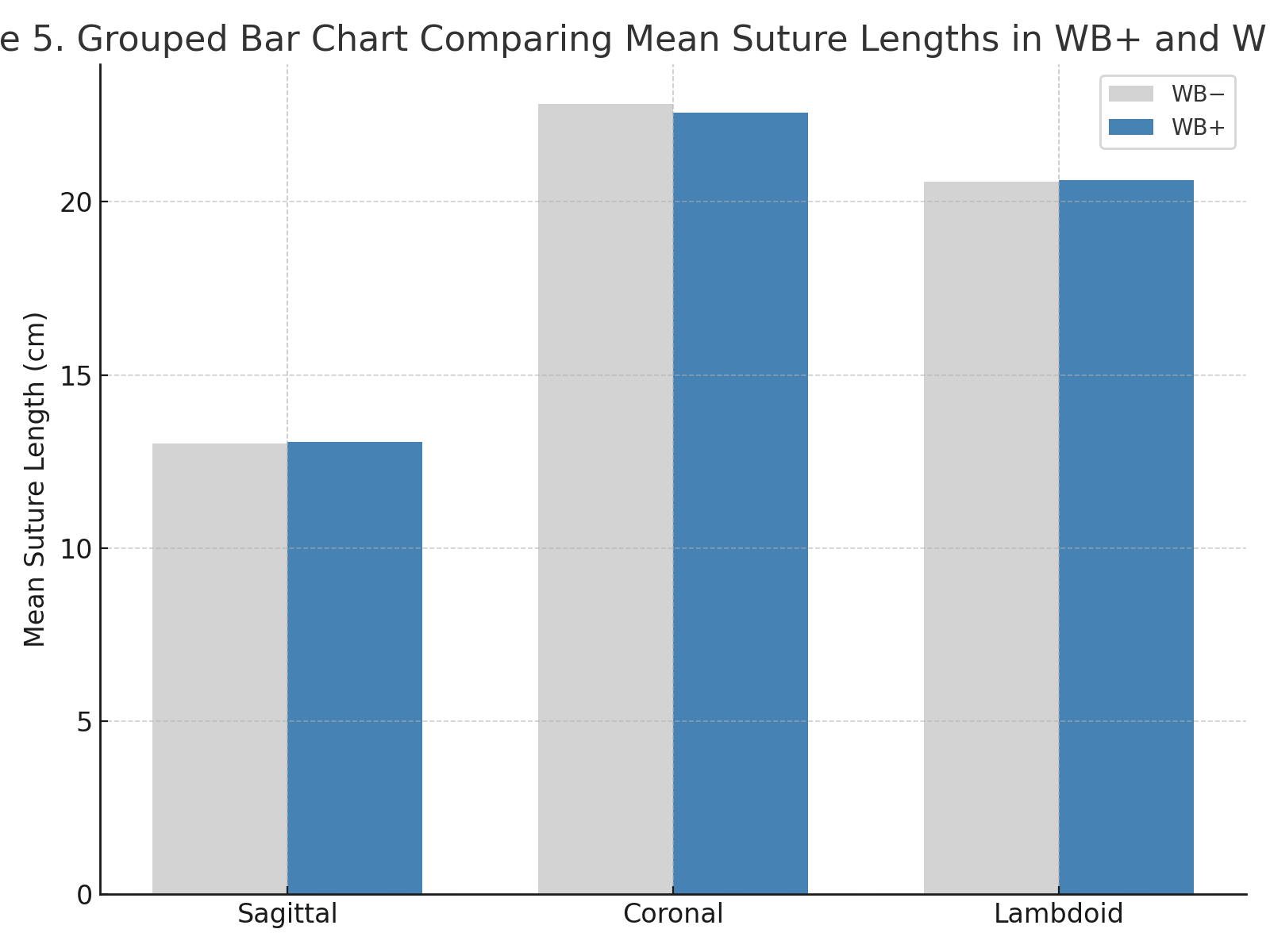
Fig. 5: Comparison of mean suture lengths in WB+vs WB− skulls
Fig. 4 Pie chart showing the shape-wise proportional distribution of Wormian bones observed in the present study. Quadrangular-shaped Wormian bones were the most common (47.76%), followed by irregular (38.81%) and triangular forms (13.43%), indicating significant morphological variability across specimens
Suture length differences between groups
Comparative analysis of cranial suture lengths was performed between skulls with (WB+) and without (WB−) Wormian bones. Although WB+skulls exhibited slightly higher mean lengths in the sagittal (13.06 cm vs 13.02 cm) and lambdoid sutures (20.64 cm vs 20.58 cm), and slightly reduced coronal length (22.58 cm vs 22.84 cm), none of these differences were statistically significant (p>0.05). The results are detailed in table 4, and the group-wise mean differences are shown in fig. 5.
Fig. 5 Grouped bar chart comparing the mean lengths of sagittal, coronal, and lambdoid sutures between skulls with (WB+) and without (WB−) Wormian bones. Although WB+skulls exhibited slightly longer sagittal and lambdoid sutures and shorter coronal sutures, none of the differences were statistically significant (p>0.05)
DISCUSSION
This anatomical investigation revealed that Wormian bones (WBs) were present in approximately half of the adult skulls analyzed, highlighting their significance as frequent cranial variants rather than rare anomalies. The study further examined their anatomical distribution, morphological patterns, and relationship with suture length in a South Indian and Andaman sample. The results add valuable region-specific morphometric data to the global understanding of these intra-sutural ossicles.
Prevalence and comparative trends
In this study, Wormian bones were observed in 48.8% of the skulls. This finding is comparable to reports from similar populations-Murlimanju et al. documented a 53.5% incidence in South Indian skulls [13], while Cirpan et al. reported a frequency of 38.6% in Turkish specimens [12]. The observed variability across regions likely reflects population-specific influences, including ethnic background, environmental factors during skull growth, and nutritional or biomechanical forces during postnatal development. The incidence in our cohort reinforces the understanding that Wormian bones are common developmental variants in the human skull.
Topographical preferences
The lambdoid suture was the most frequently involved region (16.39%), followed by the lambda (14.75%) and sagittal sutures (13.11%). This distribution is consistent with the well-documented predilection of WBs for the posterior cranial vault, particularly areas characterized by complex suture morphology and prolonged ossification [14]. The frequent occurrence at the lambda, a convergence zone for multiple cranial bones, underscores the susceptibility of this region to accessory ossification. Less frequently affected regions-such as the parietosquamous and occipitomastoid sutures-may still hold relevance in clinical and forensic scenarios, particularly in cases of multisutural involvement.
Morphological features and diagnostic relevance
The present study showed that quadrangular WBs were most common (47.76%), followed by irregular (38.81%) and triangular (13.43%) shapes. Marginal characteristics also varied, with irregular edges (59.7%) more frequently encountered than serpiginous (smoothly contoured) borders (40.3%). These results are in line with prior descriptions of suture ossicles exhibiting polymorphic outlines due to asynchronous or incomplete ossification events [15]. Such morphological variations, especially those with jagged edges, can be radiographically mistaken for cranial fractures-particularly in neonates and pediatric patients-necessitating careful differentiation by clinicians [6].
Suture length: an indicator or a coincidence?
To investigate potential morphometric correlations, suture lengths were compared between skulls with and without WBs. Although mean lengths of sagittal and lambdoid sutures were marginally longer in WB-positive specimens, and coronal lengths slightly shorter, none of these differences reached statistical significance. These findings concur with previous studies by Murlimanju et al. and Movsesian, who found no reliable association between suture dimensions and the presence of WBs [13, 16]. This suggests that while suture complexity may influence ossicle formation, linear suture length alone is not a predictive determinant.
Clinical and developmental significance
Wormian bones arise from ectopic ossification centers during intramembranous skull development and are modulated by both intrinsic genetic programming and extrinsic biomechanical forces. Although usually asymptomatic, their diagnostic importance becomes prominent in syndromic contexts. Studies have noted their increased frequency in osteogenesis imperfecta, cleidocranial dysostosis, hypothyroidism, and rickets, where multiple small ossicles may cluster along the lambdoid suture [7, 8]. Importantly, none of the specimens in the present study displayed overt cranial pathology, supporting the view that WBs are benign anatomical variations in otherwise normal individuals.
In radiologic practice, WBs can resemble fracture lines or suture diastasis. Their common occurrence in the lambdoid region may complicate posterior fossa imaging interpretations. Radiologists must recognize their typical appearances to avoid misdiagnosis, particularly in medicolegal or trauma settings [6]. Furthermore, these ossicles may disrupt anticipated cranial contours during neurosurgical procedures, especially near the posterior fontanelle or asterion, potentially altering burr hole or craniotomy planning [7].
Anthropological and forensic considerations
From an anthropological perspective, the presence, number, and configuration of WBs can offer clues to ancestry, population migration, and epigenetic trends. As non-metric cranial traits, their documentation contributes to osteological profiling in forensic anthropology [3, 9]. In the absence of demographic data such as age or sex in this study, population-level comparisons remain limited. Nevertheless, the site-specific trends observed here could aid in refining regionally relevant cranial morphometry datasets.
Study limitations and scope for future work
This study is limited by its retrospective design and the lack of demographic metadata for the specimens analyzed. Furthermore, the reliance on gross anatomical measurements may overlook microstructural or histologic nuances in suture development. Future research incorporating high-resolution imaging (e. g., CT or 3D surface scanning) and histological analysis may clarify the developmental biology of WBs and their biomechanical underpinnings. Multicentric studies with larger samples and known demographic variables would also strengthen population-level inferences.
CONCLUSION
Wormian bones were commonly identified in the present South Indian and Andaman sample, with a strong preference for the lambdoid and lambda sutures. While morphologically diverse, their presence was not associated with significant alterations in cranial suture length. Recognizing their anatomical and radiologic features is essential for clinicians, surgeons, and forensic experts to avoid diagnostic pitfalls and deepen understanding of calvarial development.
ACKNOWLEDGEMENT
The authors are grateful to the Departments of Anatomy at ANIIMS, Port Blair, and A. J. Institute of Medical Sciences and Research Centre, Mangaluru, for their academic support and for granting access to osteological materials necessary for this research.
FUNDING
No financial support was received from any governmental, private, or non-profit funding agency for the execution of this study.
AUTHORS CONTRIBUTIONS
Dr. Ashok Pal Gobind: Conceptualization, data acquisition, morphological analysis, manuscript preparation
Dr. Vidya R. Pillai: Cranial suture measurements, data organization, manuscript revision
Dr. Rituraj Majumder: Statistical analysis, preparation of tables and figures, literature synthesis
Dr. Arbind Kumar Choudhary (Corresponding Author): Supervision, anatomical interpretation, final manuscript approval
All authors have read and approved the final manuscript.
CONFLICTS OF INTERESTS
The authors declare that there are no conflicts of interest related to the content of this manuscript.
REFERENCES
Cruveilhier J. The anatomy of the human body. In: Pattison GS, editor. Philadelphia: lea and Blanchard; 1844.
Masih WF, Gupta S, Chand AE, Jaiswal P, Saraswat PK. Incidence of wormian bone in human skulls in Rajasthan. J Evol Med Dent Sci. 2013;2(9):1007-12. doi: 10.14260/jemds/370.
Berry RJ. Section I. Genes and skeletons ancient and modern. J Hum Evol. 1979;8(7):669-77. doi: 10.1016/0047-2484(79)90067-8.
Pryles CV, Khan AJ. Wormian bones a marker of CNS abnormality? Am J Dis Child. 1979;133(4):380-2. doi: 10.1001/archpedi.1979.02130040034007, PMID 433853.
Liu YH, Tang Z, Kundu RK, Wu L, Luo W, Zhu D. Msx2 gene dosage influences the number of proliferative osteogenic cells in growth centers of the developing murine skull: a possible mechanism for MSX2-mediated craniosynostosis in humans. Dev Biol. 1999;205(2):260-74. doi: 10.1006/dbio.1998.9114, PMID 9917362.
Jeanty P, Silva SR, Turner C. Prenatal diagnosis of wormian bones. J Ultrasound Med. 2000;19(12):863-9. doi: 10.7863/jum.2000.19.12.863, PMID 11127012.
Graham JM JR, Kreutzman J, Earl D, Halberg A, Samayoa C, Guo X. Deformational brachycephaly in supine sleeping infants. J Pediatr. 2005;146(2):253-7. doi: 10.1016/j.jpeds.2004.10.017, PMID 15689919.
Bhanu PS, Sankar KD. Interparietal and pre-interparietal bones in the population of south coastal Andhra Pradesh, India. Folia Morphol (Warsz). 2011;70(3):185-90. PMID 21866530.
Srivastava HC. Ossification of the membranous portion of the squamous part of the occipital bone in man. J Anat. 1992;180(2):219-24. PMID 1506277, PMCID PMC1259666.
Walulkar S, Ksheersagar D, Walulkar M. The study of wormian bones in human skulls in Vidarbha region. Pak J Med Sci. 2012;2(2):18-21.
Singh R. Incidence of sutural bones at Asterion in adults Indians skulls. Int J Morphol. 2012;30(3):1182-6. doi: 10.4067/S0717-95022012000300066.
Cirpan S, Aksu F, Mas N, Magden AO. Coexistence of wormian bones with metopism and vice versa in adult skulls. J Craniofac Surg. 2016;27(2):493-5. doi: 10.1097/SCS.0000000000002370, PMID 26845093.
Murlimanju BV, Prabhu LV, Ashraf CM, Kumar C, Rai R, Maheshwari C. Morphological and topographical study of wormian bones in cadaver dry skulls. J Morphol Sci. 2011;28(3):176-9.
Bellary SS, Steinberg A, Mirzayan N, Shirak M, Tubbs RS, Cohen Gadol AA. Wormian bones: a review. Clin Anat. 2013;26(8):922-7. doi: 10.1002/ca.22262, PMID 23959948.
Marti B, Sirinelli D, Maurin L, Carpentier E. Wormian bones in a general paediatric population. Diagn Interv Imaging. 2013;94(4):428-32. doi: 10.1016/j.diii.2013.01.001, PMID 23352712.
Govsa F, Ozer MA, Bayraktaroglu S, Aktas EO. Anatomoradiological identification of intrasutural bones for importance of cranial fracture. Turk Neurosurg. 2014;24(3):357-62. doi: 10.5137/1019-5149.JTN.8380-13.2, PMID 24848174.
Khan AA, Asari MA, Hassan A. Unusual presence of wormian (sutural) bones in human skulls. Folia Morphol (Warsz). 2011;70(4):291-4. PMID 22117248.