
Int J Curr Pharm Res, Vol 17, Issue 4, 124-126Case Study
BENIGN PHYLLODES TUMOR ARISING IN AXILLARY BREAST TISSUE; A RARE CASE WITH AVAILABLE REVIEW OF LITERATURE
MONICA DASH1, PRAGNYA PARAMITA MISHRA2*, PREMANAND PANDA3
1,2Department of Pathology, Hi-Tech MCH, Rourkela, Odisha, India. 3Department of Radiology, JP Hospital and Research Centre, Rourkela, Odisha, India
Email: panda.premanand@gmail.com
Received: 18 Apr 2025, Revised and Accepted: 14 Jun 2025
ABSTRACT
Anatomical variation known as accessory breast tissue arises during embryogenic development. The axilla is where it most commonly occurs. Accessory breast tissue may experience both benign and malignant processes similar to those in normal breast tissue. We describe a 40-year-old woman who had a palpable mass at her left axilla and who later developed a benign phyllodes tumor in her axillary breast tissue. Microscopy revealed an encapsulated tumor composed of cells arranged in singles, compressing the epithelial cells into a leaf-like (phyllodes) pattern with a mild lymphocytic stromal response. Although phyllodes tumors in axillary breast tissue are a very uncommon occurrence, this case study provided additional information on the tumor, which might promote improvements in disease management.
Keywords: Axillary breast tissue, Fibroadenoma, Phyllodes tumor
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i4.7029 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
An unusual hormone-responsive deviation from normal breast development, accessory breast tissue experiences physiological and pathological alterations that are comparable to those of regular breast tissue. According to reports, the prevalence of accessory breast tissue in the general population ranges from 2% to 6%, with women having a significantly higher prevalence [1]. With far less frequent occurrences in the thorax, abdomen, inguinal region, and vulva, it is mainly found in the axilla [2]. Among the pathologies are inflammatory conditions and a range of benign and malignant tumors that might present diagnostic challenges and are frequently undiagnosed clinically. Here, we report an extremely rare case of a benign phyllodes tumor growing in the left axillary accessory breast tissue of a lady aged 40.
CASE REPORT
A 40 y old female presented with a palpable mass at the left axilla, which had been present for a month with rapid growth. Breast ultrasound showed a huge mass with lobulated borders and internal cystic clefts at the left axilla with an approximate size of 10.0 x 9.0 x 9.0 cm (fig. 1).
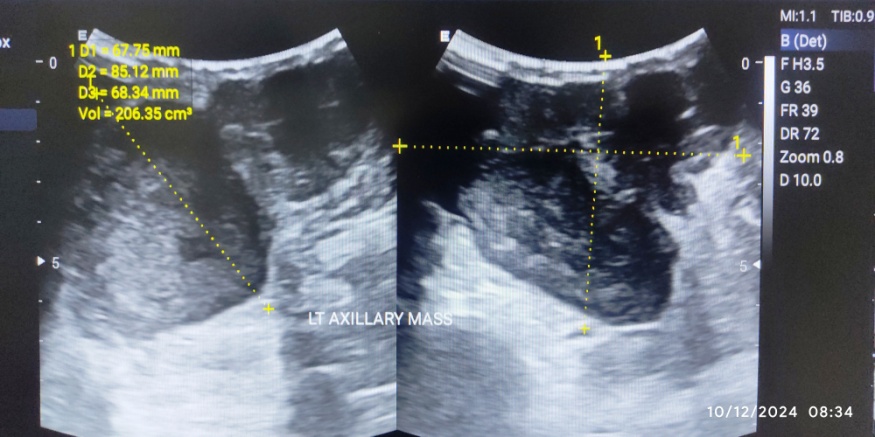
Fig. 1: Ultrasonography image showing huge mass with lobulated borders and internal cystic clefts with an approximate size of 10.0 x 9.0 x 9.0 cm at the left axilla
On FNAC, smears showed benign duct epithelial cells along with myoepithelial cells arranged in small clusters with many bipolar bare nuclei with few stromal fragments, prompting a diagnosis suggestive of benign breast disease. With proper pre-surgical workup, the mass was excised and sent to the pathology department. Gross examination showed a skin-covered excised specimen measuring 10.0 x 9.0 x 9.0 cm, and its cut surface revealed a tumor measuring 9.6 x 8.5 x 8.5 cm, which was grey-white and firm. Cut sections of the tumor showed myxoid areas (fig. 2).
Histopathological sections studied showed stratified squamous epithelium with underlying capsulated neoplasm with cells arranged in singles, compressing the epithelial cells into a leaf-like epithelial pattern (fig. 3). Cells exhibited mild pleomorphism and scattered mitosis. Mild lymphocytic stromal response with no increased stromal atypia was seen. Also, two reactive lymph nodes were noted. These findings are compatible with benign phyllodes tumor.

Fig. 2: Gross photograph of tumour measuring 9.6 x 8.5 x 8.5 cm, cut surface of tumour is grey-white and firm with myxoid areas
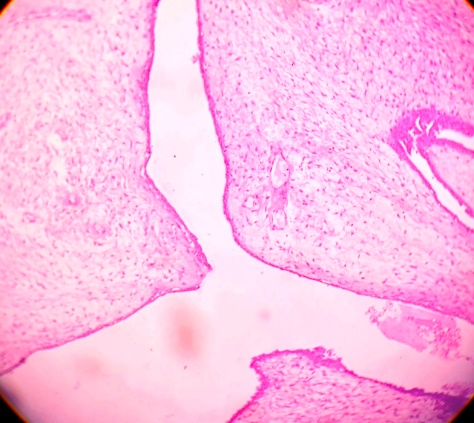
Fig. 3: Microscopic photograph of tumour showing epithelial cells arranged in leaf-like pattern with surround spindle cells
DISCUSSION
Remaining breast tissue from normal embryologic development is referred to as accessory breast tissue. It usually happens along the bilateral milk line, which runs from the medial thigh and inguinal regions to the anterior axillary folds. The axilla is where supplementary breast tissue is most frequently found [3]. A patient with accessory breast tissue may be asymptomatic or exhibit a palpable lump in the axilla. Normal breast tissue that reacts to hormones is the same as accessory breast tissue. Understanding accessory breast tissue is crucial for enhancing the standard of patient care because the diagnosis might be mistaken for a number of disorders, such as lymphadenopathy, lipoma, vascular malformation, or cancer. The pathophysiology of benign and malignant cancers that can develop in accessory breast tissue is crucial to resolving this issue [1, 3, 4]. Women between the ages of 30 and 40 are most likely to have benign proliferative breast lesions, which can occasionally result in severe breast asymmetry because of their size. Benign phyllodes tumors, juvenile fibroadenomas, large fibroadenomas with enhanced stromal cellularity, and pseudoangiomatous stromal hyperplasia (PASH) are among the differential diagnoses for these lesions [5]. Rare fibroepithelial breast cancers are called phyllodes tumors. Although the tissue's histopathology shows a typical leaf-like protrusion and enhanced stromal hypercellularity, its structural pathology is comparable to that of fibroadenoma.
Histopathological, radiographic, and clinical examination are used to evaluate phyllodes tumors [6, 7]. The World Health Organization's 2003 guidelines serve as the basis for diagnosing phyllodes tumors. Three histological categories are used to classify phyllodes tumors: benign, borderline, and malignant [8] (table 1).
Table 1: Comparing histopathologic features of benign, borderline and malignant phyllodes tumors [8]
| Histologic features | Benign phyllodes | Boderline phyllodes | Malignant phyllodes |
| Tumor border | Well defined | Well defined, may be focal permeative | Permeative |
| Stromal cellularity | Cellular, usually mild, may be non-uniform or diffuse | Cellular, usually moderate, may be non-uniform or diffuse | Cellular, usually marked and diffuse |
| Stromal atypia | Mild or none | Mild or moderate | Marked |
| Mitotic activity | Usually low: | Usually frequent: | Usually abundant: |
| <5 per 10 HPFs | 5-9 per 10 HPFs | ≥10 per 10 HPFs | |
| Stromal overgrowth | Absent | Absent (or very focal) | Often present |
| Malignant heterologous elements | Absent | Absent | Maybe present |
| Relative proportion of all phyllodes tumor | 60%-75% | 15%-26% | 8%-20% |
Phyllodes tumors that develop in ectopic breast tissue are extremely uncommon. They have usually been observed in the axilla and vulva. According to a review of the literature, there are only six examples of axilla (excluding the current case) [9-13].
Each diagnostic group has its own set of surgical treatment guidelines for proliferative breast lesions. Except for phyllodes tumors, which make up 2.5% of fibroepithelial lesions, fibroepithelial lesions are benign [14]. Clinical signs such as advanced age and a big tumor with a history of rapid growth may raise the suspicion of phyllodes tumors. Preoperative tissue identification and surgical methods for breast rebuilding following tumor excision are crucial aspects of managing phyllodes tumors.
Excision of the lesion with wide margins is the standard treatment for phyllodes tumors. According to a number of papers, phyllodes tumors should have margins of at least 1 cm. Since local recurrence typically happens within the first few years after surgery, particularly if the excision was partial, the prognosis for phyllodes tumors can be significantly improved [5-7, 15]. When the tumors are big or larger, excision by total enucleation may be necessary, particularly in women over 35 [15, 16].
CONCLUSION
The present study reports a benign phyllodes tumor in axillary breast tissue, which is extremely rare and is misdiagnosed owing to the diagnostic complexity. In conclusion, the diagnosis, treatment, and prognostic details of the tumor presented in the case report will assist in improving further knowledge of the characteristics of this less-known, rarely diagnosed entity.
PATIENT CONSENT
Written informed consent was obtained from the patient for the publication of this case report.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICTS OF INTERESTS
There are no conflicts of interest.
REFERENCES
Znagui I, Olfa S, Moez A, Riadh BT, Taher M, Nabil M. Malignant phyllodes tumor in ectopic breast tissue: a case report with a literature review. Arch Can Res. 2018;6(1):1. doi: 10.21767/2254-6081.100167.
Go JH. Cystic benign phyllodes tumor in the inguinal region. Korean J Pathol. 2013;47(6):583-6. doi: 10.4132/KoreanJPathol.2013.47.6.583, PMID 24421854.
EM De Filippis, EK Arleo. The ABCs of accessory breast tissue: basic information every radiologist should know. AJR Am J Roentgenol. 2014 May;202(5):1157-62. doi: 10.2214/AJR.13.10930.
Laporte BE, Salgado HC, Monteza NM, Rangel JM, Carvalho MA, Esperanca SD. Fibroadenoma in axillary accessory breast: a case report. Braz Soc Mastol; 2020. p. 1-4.
Chirappapha P, Lertsithichai P, Sukarayothin T, Leesombatpaiboon M, Supsamutchai C, Kongdan Y. Kondan oncoplastic techniques in breast surgery for special therapeutic problems. Gland Surg. 2016;5(1):75-82. doi: 10.3978/j.issn.2227-684X.2015.05.04, PMID 26855912.
Krairittichai U, Sethakarun S. A randomized controlled trial of seroconversion after 20 mg versus 40 mg intramuscular hepatitis b virus vaccination in patients with chronic kidney disease stage 3. J Med Assoc Thai. 2017;100 Suppl 1:S1-7. doi: 10.1016/S0960-9776(19)30418-7, PMID 29926711.
Pornchai S, Chirappapha P, Pipatsakulroj W, Lertsithichai P, Vassanasiri W, Sitathanee C. Malignant transformation of phyllodes tumor: a case report and review of literature. Clin Case Rep. 2018 Feb 25;6(4):678-85. doi: 10.1002/ccr3.1428, PMID 29636939.
Tan PH, Ellis I, Allison K, Brogi E, Fox SB, Lakhani S. The 2019 World Health Organization classification of tumours of the breast. Histopathology. 2020 Aug;77(2):181-5. doi: 10.1111/his.14091, PMID 32056259.
Saleh HA, Klein LH. Cystosarcoma phyllodes arising synchronously in right breast and bilateral axillary ectopic breast tissue. Arch Pathol Lab Med. 1990;114(6):624-6. PMID 2161206.
Oshida K, Miyauchi M, Yamamoto N, Takeuchi T, Suzuki M, Nagashima T. Phyllodes tumor arising in ectopic breast tissue of the axilla. Breast Cancer. 2003;10(1):82-4. doi: 10.1007/BF02967630, PMID 12525768.
Ruvalcaba Limon E, Bautista Pina V, Ramirez Bollas J, Espejo Fonseca R, Rodriguez Cuevas S. A nonpalpable nodule in ectopic axillary breast tissue: consider phyllodes tumor. Case Rep Pathol. 2016;2016:3603262. doi: 10.1155/2016/3603262, PMID 28105378.
R Zubair. Phyllodes tumor arising in the ectopic breast tissue of axilla a rare pathology. Cancer Biol Ther Oncol. 2020;4:9.
Fujimoto A, Matsuura K, Hasebe T, T Saeki. Phyllodes tumor arisning in the ectopic axillary breast tissue mimicking axillary lymphadenopathy. BMJ Case Rep. 2021 May 26;14(5):1-2. doi: 10.1136/bcr-2021-243341.
Kim JH, Lee JY. Malignant phyllodes tumor of the breast with liposarcomatous differentiation: a case report with imaging findings. Radiol Case Rep. 2019;14(5):531-4. doi: 10.1016/j.radcr.2019.02.007, PMID 30834064.
Jacklin RK, Ridgway PF, Ziprin P, Healy V, Hadjiminas D, Darzi A. Optimising preoperative diagnosis in phyllodes tumour of the breast. J Clin Pathol. 2006;59(5):454-9. doi: 10.1136/jcp.2005.025866, PMID 16461806.
Cerrato F, Labow BI. Diagnosis and management of fibroadenomas in the adolescent breast. Semin Plast Surg. 2013;27(1):23-5. doi: 10.1055/s-0033-1343992, PMID 24872735.