
Int J Curr Pharm Res, Vol 17, Issue 6, 36-39Original Article
COMPARISON BETWEEN ISOFLURANE AND SEVOFLURANE IN THE MAINTENANCE OF HYPOTENSIVE ANAESTHESIA IN ENDOSCOPIC SINUS SURGERIES
KOTHAPALLI TEJA SRI RAKESH1*, NANNA VARUN KOUSHIK2, RATHNAPURAM LAXMAN1
1Department of Anaesthesiology, Government Medical College and General Hospital, Sangareddy, Telangana, India. 2Department of Emergency Medicine, Government Medical College and General Hospital, Mahabubabad, Telangana, India
*Corresponding author: Kothapalli Teja Sri Rakesh; *Email: ktsrakesh@gmail.com
Received: 14 Aug 2025, Revised and Accepted: 02 Oct 2025
ABSTRACT
Objective: To compare the efficacy of isoflurane and sevoflurane in maintaining controlled hypotensive anesthesia during ESS, focusing on intraoperative hemodynamics, blood loss, surgical field quality, recovery profile, and postoperative pain.
Methods: This prospective randomized study included 80 ASA I/II patients aged 18–60 undergoing elective ESS. Patients were divided into two groups: Group I received isoflurane and Group S received sevoflurane. Hemodynamic parameters (MAP, HR), blood loss, surgical field visibility, recovery times, and postoperative pain (VAS scores) were recorded and analyzed statistically.
Results: Sevoflurane significantly maintained lower MAP and HR during surgery (p<0.05) and was associated with reduced intraoperative blood loss (110.6±18.9 ml vs. 135.2±20.3 ml; p = 0.001) and improved surgical field scores (p = 0.002). Recovery was faster in Group S across all parameters, including eye opening, extubation, and orientation (p<0.001). Postoperative pain scores were consistently lower in the sevoflurane group during the early recovery period (p<0.05).
Conclusion: Sevoflurane proved superior to isoflurane in achieving controlled hypotension, reducing blood loss, improving the surgical field, enhancing recovery profile, and minimizing early postoperative pain in patients undergoing ESS. It is therefore a preferred agent for maintaining hypotensive anesthesia in such procedures.
Keywords: Sevoflurane, Isoflurane, Endoscopic sinus surgery, Hypotensive anaesthesia
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i6.7066 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Endoscopic sinus surgery (ESS) is a widely accepted, minimally invasive surgical technique used to manage chronic rhinosinusitis and other sinonasal pathologies [1]. The success of ESS depends significantly on optimal visualization of the surgical field, which can be compromised by even minimal bleeding due to the narrow and vascular nature of the nasal and paranasal sinus cavities. Hence, one of the key anesthetic goals during ESS is to provide a controlled hypotensive environment to reduce intraoperative bleeding, thereby improving the surgeon’s view and overall surgical outcome.
The estimated global pooled prevalence of sinusitis is 8.71%. Chronic rhinosinusitis with nasal polyps (CRSwNP) has a reduced prevalence, estimated to be 0.65% worldwide [2]. Chronic rhinosinusitis (CRS) impacts 1 in 8 individuals in India; approximately 5-15% of the urban population. The occurrence of sinusitis (146 per 1000 population) has been indicated to surpass that of any other long-term state and seems to be rising [3].
Hypotensive Anaesthesia was first introduced by Cushing in 1917, and it was first used in nasal surgeries by Gardner in 1946 [4]. Controlled hypotensive anesthesia is a deliberate reduction in the patient’s systemic blood pressure to a level that reduces surgical bleeding without compromising vital organ perfusion. Generally, the mean arterial pressure (MAP) is lowered to 55–65 mmHg or approximately 30% below the patient’s baseline. This technique not only reduces blood loss but also shortens the duration of surgery, enhances precision, and improves patient safety. Multiple pharmacological agents including inhalational anesthetics, intravenous agents, vasodilators, and beta-blockers can be employed to achieve controlled hypotension.
Among the various methods available, inhalational agents play a central role in both maintenance of general anesthesia and achieving controlled hypotension. Volatile anesthetics offer the advantage of easy titratability, rapid onset and offset (depending on their solubility), and predictable hemodynamic effects. Two of the most commonly used agents in this context are isoflurane and sevoflurane [5]. Both are halogenated ethers with vasodilatory properties, but they differ in their pharmacokinetic and pharmacodynamic profiles, which may impact their efficacy in providing an ideal surgical field during ESS.
Isoflurane is a widely used inhalational anesthetic known for its cardiovascular stability and long duration of action. It produces hypotension primarily by reducing systemic vascular resistance while maintaining cardiac output [6]. However, it has a higher blood-gas partition coefficient, resulting in slower induction and recovery compared to newer agents. Despite this, it remains in use due to its cost-effectiveness, predictable depth of anesthesia, and long-standing safety profile.
Sevoflurane is a another inhalational agent with a low blood-gas partition coefficient, offering rapid induction and emergence from anesthesia. It provides dose-dependent hypotension, largely through myocardial depression and peripheral vasodilation. Sevoflurane is often preferred in short procedures or outpatient settings due to its smooth induction and rapid postoperative recovery [7, 8]. Additionally, it is associated with a lower pungency, making it suitable for inhalational induction in both pediatric and adult patients.
Given the need for fine surgical precision during ESS, the choice between isoflurane and sevoflurane may significantly influence operative conditions. Various clinical trials have compared these agents in terms of their efficacy in achieving controlled hypotension, intraoperative bleeding, surgeon satisfaction scores, emergence time, and adverse effects.
MATERIALS AND METHODS
This randomized comparative study was conducted prospectively for a period of 1 year at a Rural Hospital in South India, with ethical approval granted by the institutional review board. A total of 80 patients, aged 18 to 60, who were classified as ASA I or II and scheduled to undergo elective endoscopic sinus surgery, were recruited after providing informed consent. Patients were randomly assigned to two groups of 40 individuals each:
1. Group I (n = 40): Received isoflurane for maintenance of hypotensive anaesthesia.
Group S (n = 40): Received sevoflurane for maintenance of hypotensive anaesthesia.
Inclusion criteria
Patients aged between 18 and 60 y
ASA physical status I or II
Electively scheduled for endoscopic sinus surgery
Patients who provided informed written consent
Exclusion criteria
Patients with history of significant cardiac, pulmonary, hepatic, renal, or hematological disease
Patients who had allergy to anaesthetic agents
Presence of nasal polyposis or bleeding disorders
Bronchial asthma or uncontrolled hypertension
Patients on chronic antihypertensive medication
Methodology
Every patient received a standard preoperative assessment. Anaesthesia was initiated using propofol (2 mg/kg), fentanyl (1 µg/kg), and rocuronium (0.6 mg/kg). After endotracheal intubation, the lungs were mechanically ventilated to maintain an end-tidal carbon dioxide level between 25 and 35 mm Hg. Anaesthesia was sustained with either isoflurane or sevoflurane in a 50:50 mixture of oxygen and nitrous oxide (3 l/min), adjusted to keep MAP 20–30% under baseline levels.
Nasal infiltration with epinephrine at a concentration of 1:100,000 was performed prior to the incision. Standardized surgical methods and Merocel nasal packing were implemented. At the conclusion of the surgery, anaesthetic agents were stopped, and neuromuscular blockade was reversed using neostigmine and atropine.
Parameteres recorded included intraoperative blood loss, heart rate, mean arterial pressure (MAP), duration of surgery, recovery time, and postoperative pain scores (VAS at 1, 3, 5, 12, 16, and 24 h).
Statistical analysis
Data were inputted into Microsoft Excel and examined using SPSS version 25. Continuous variables were represented as mean±standard deviation and analyzed utilizing Student's t-test. Categorical variables were analyzed using the chi-square test. A p-value less than 0.05 was considered statistically significant.
Observations and results
Table 1 indicates that both groups were comparable regarding age, gender, weight, and ASA classification, with no statistically significant differences (p>0.05), confirming equivalent baseline characteristics.
Table 1: Demographic profile of patients
| Parameter | Group I (Isoflurane) | Group S (Sevoflurane) | p-value |
| Age (years) | 38.2±10.5 | 37.6±9.8 | 0.71 |
| Gender (M/F) | 22/18 | 20/20 | 0.65 |
| Weight (kg) | 66.3±8.4 | 65.7±7.9 | 0.78 |
| ASA I/II | 30/10 | 28/12 | 0.62 |
Table 2 shows that Sevoflurane maintained lower mean arterial pressure and heart rate during the surgery in comparison to Isoflurane, with significant differences observed at 30 min (p<0.05 for both MAP and HR).
Table 2: Hemodynamic parameteres during surgery
| Time point | MAP (mmHg) group I | MAP (mmHg) group S | HR (bpm) group I | HR (bpm) group S | p-value (MAP/HR) |
| Baseline | 92.1±6.8 | 91.7±7.1 | 81.5±5.3 | 80.8±6.1 | 0.74/0.60 |
| 15 min | 68.3±5.6 | 66.2±5.1 | 75.2±4.8 | 72.6±5.0 | 0.04/0.03 |
| 30 min | 66.9±4.9 | 64.3±4.7 | 73.4±5.0 | 70.5±4.9 | 0.03/0.01 |
| 45 min | 67.8±4.7 | 65.1±4.5 | 72.8±4.7 | 70.1±4.4 | 0.02/0.01 |
Table 3 shows that patients who received Sevoflurane experienced less intraoperative blood loss and enhanced visibility during surgery with statistically signifcant p-value of<0.05, respectively.
Table 3: Intraoperative parameteres between groups
| Parameter | Group I (Isoflurane) | Group S (Sevoflurane) | p-value |
| Duration of surgery (min) | 72.4±10.6 | 70.1±9.8 | 0.27 |
| Blood loss (mL) | 135.2±20.3 | 110.6±18.9 | 0.001 |
| Surgical field score (1–5) | 2.8±0.6 | 2.3±0.5 | 0.002 |
Table 4 and fig. 1 indicate shorter recovery duration in the Sevoflurane group, with faster responses such as eye opening, extubation, and orientation, with significant statistical difference of p value<0.05.
Table 4: Recovery profile of patients
| Parameter | Group I (Isoflurane) | Group S (Sevoflurane) | p-value |
| Time to eye opening (min) | 9.6±2.2 | 6.2±1.8 | <0.001 |
| Time to extubation (min) | 11.3±2.5 | 7.9±2.1 | <0.001 |
| Time to orientation (min) | 13.2±2.7 | 9.6±2.3 | <0.001 |
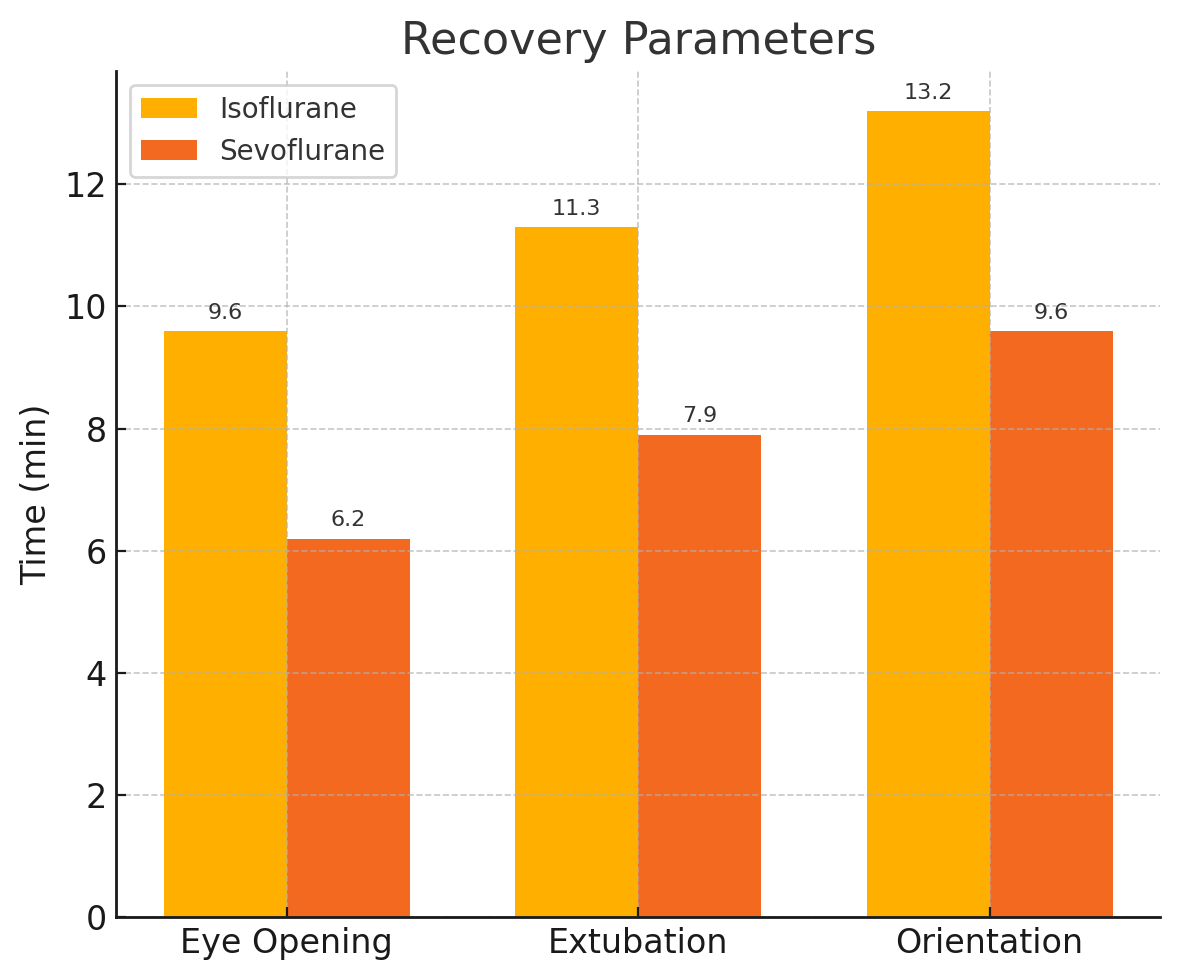
Fig. 1: Recovery profile of patients
Table 5: Post-operative pain scores (VAS scale)
| Time post-Op | Group I (isoflurane) | Group S (sevoflurane) | p-value |
| 1 hour | 4.6±1.2 | 3.8±1.1 | 0.01 |
| 3 h | 3.9±1.1 | 3.2±0.9 | 0.01 |
| 5 h | 3.5±1.0 | 2.8±0.8 | 0.008 |
| 12 h | 2.6±0.8 | 2.1±0.7 | 0.03 |
| 24 h | 1.9±0.7 | 1.6±0.6 | 0.06 |
Table 5 demonstrates that postoperative pain was consistently reduced in the Sevoflurane group during the initial recovery period, showing significant declines at 1, 3, and 5 h (p<0.05), but scores were comparable by 24 h (p = 0.06).
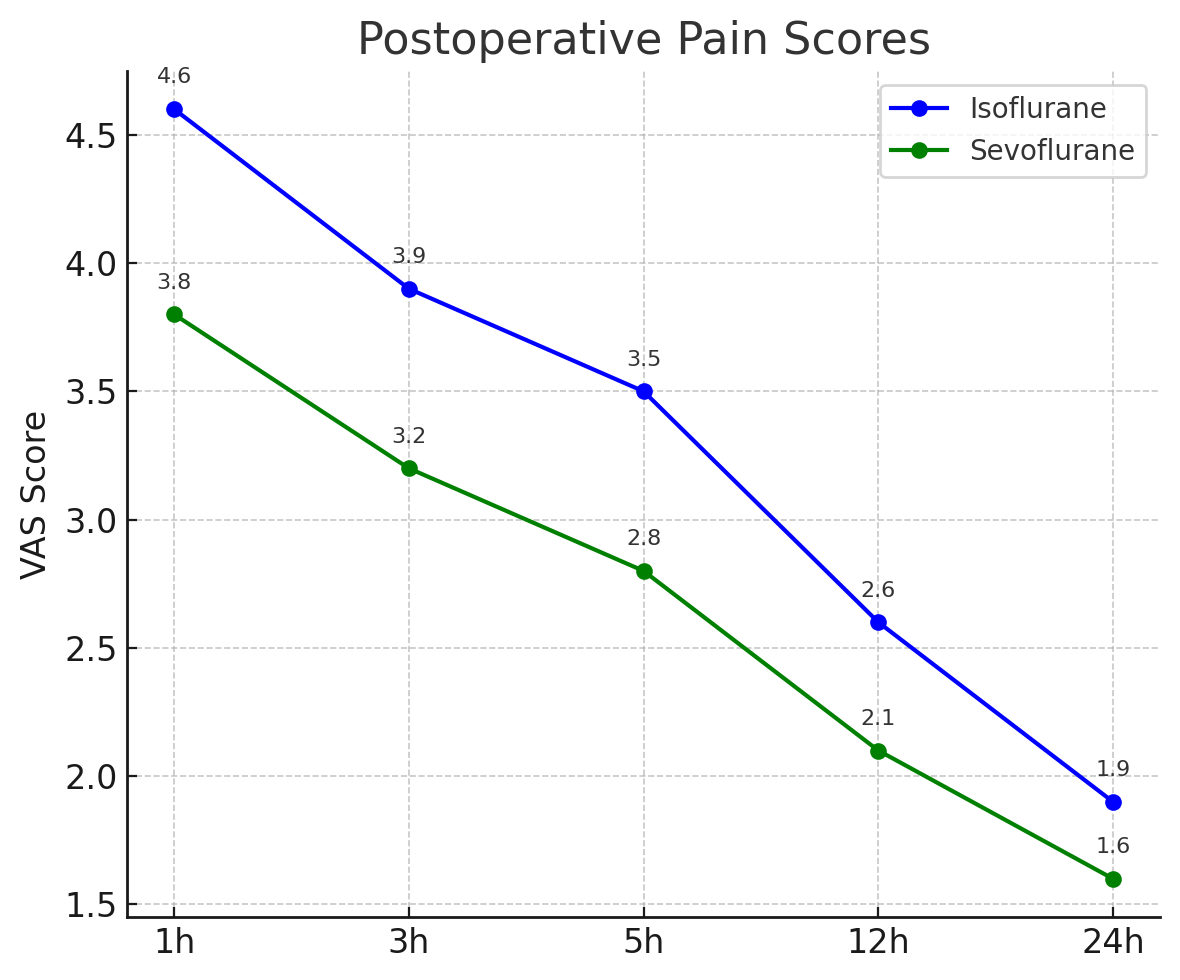
Fig. 2: Post-operative pain scores (VAS scale)
DISCUSSION
The present study compared the effectiveness of isoflurane and sevoflurane in the maintenance of hypotensive anaesthesia during endoscopic sinus surgery. The average age was 38.2±10.5 y in Group I and 37.6±9.8 y in Group S. Gender distribution (M/F: 22/18 vs. 20/20), weight (66.3±8.4 kg vs. 65.7±7.9 kg), and ASA I/II classification (30/10 vs. 28/12) revealed no significant differences (p-value>0.05), verifying that both groups were similar at baseline. Similarly, in the study conducted by Behzad Ahsan et al. in 2022 [9], 46 surgical patients were split into two groups: Sevoflurane (n=23) and Isoflurane (n=23). The Sevoflurane group comprised notably younger individuals (33.96±3.67 y vs. 43.3±3.67; p = 0.015) and had a lower body weight (p = 0.015), while there were no differences in height or bleeding rates (p>0.05) which also aligns with our results.
Intraoperative hemodynamic assessment showed that Group S sustained markedly lower mean arterial pressure (MAP) and heart rate (HR) throughout the procedure which closely aligns with the Behzad Ahzan et al. study [9] where baseline systolic and diastolic blood pressures were notably reduced in the Sevoflurane group (p = 0.03 and p = 0.009, respectively). In our study, at 30 min, MAP measured 66.9±4.9 mmHg in Group I and 64.3±4.7 mmHg in Group S (p = 0.03), whereas HR was 73.4±5.0 bpm compared to 70.5±4.9 bpm with staitistically significant value of<0.05. These results support that sevoflurane was superior in attaining and maintaining controlled hypotension.
Intraoperative metrics additionally supported sevoflurane: average blood loss was notably reduced in Group S (110.6±18.9 ml) versus Group I (135.2±20.3 ml), yielding a p-value of<0.05. Group S demonstrated improved surgical field visibility, with an average score of 2.3±0.5 compared to 2.8±0.6 in Group I, suggesting more favorable operative conditions when using sevoflurane. In contrast, Sivaci et al. in 2004 [10] analysed the influence of propofol and sevoflurane anesthesia on intraoperative bleeding in endoscopic sinus surgery. The findings revealed no notable differences in surgery duration or mean arterial pressure between the two groups. The average blood loss was considerably greater in the sevoflurane group (296.9±97.8 ml) than in the propofol group (128.1±37.3 ml), with a p-value of<0.01, suggesting that propofol was superior in reducing surgical bleeding under similar conditions.
Recovery times were notably reduced in Group S for all parameters. Time to eye opening was 6.2±1.8 min compared to 9.6±2.2 min, time to extubation was 7.9±2.1 vs. 11.3±2.5 min), and time to orientation was 9.6±2.3 vs. 13.2±2.7 min with a statistical significance of p<0.05. These findings suggest a quicker and more seamless recovery from anaesthesia when using sevoflurane. These results aligns with the Cantillo et al.'s (1997) [11] findings where sevoflurane was associated with a significantly faster emergence from anaesthesia compared to isoflurane (5.6 vs. 11.2 min), although no significant differences were noted in extubation time, response to verbal commands, or orientation. Hence, both studies support the advantage of sevoflurane in facilitating quicker recovery after surgery.
Postoperative pain scores (VAS) were considerably reduced in Group S during the initial recovery phase. At 1 hour, pain ratings were 3.8±1.1 for Group S compared to 4.6±1.2 for Group I, and at 5 h, they were 2.8±0.8 versus 3.5±1.0. At 24 h, pain scores aligned (1.6±0.6 vs. 1.9±0.7; p<0.05), indicating no notable difference. This indicates improved early postoperative pain relief with sevoflurane. Similarly, Özkiris et al. [8] found that the average pain score post-surgery from 1 to 24 h after endoscopic sinus surgery in their study was significantly reduced in the sevoflurane group (3.4±0.5) versus the isoflurane group (4.5±1.2), with a statistically significant difference.
CONCLUSION
In conclusion, Sevoflurane proved to be more effective than Isoflurane for sustaining controlled hypotensive anaesthesia throughout endoscopic sinus surgery. It offered enhanced intraoperative hemodynamic stability, decreased blood loss, and better visibility in the surgical field. Recovery durations were notably reduced, and initial postoperative pain ratings were less with sevoflurane. These results correspond with earlier studies, reinforcing its advantages for improved surgical and recovery results.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCES
Messerklinger W. Technics and possibilities of nasal endoscopy. HNO. 1972 May;20(5):133-5. PMID 5049779.
Min HK, Lee S, Kim S, Son Y, Park J, Kim HJ. Global incidence and prevalence of chronic rhinosinusitis: a systematic review. Clin Exp Allergy. 2025 Jan;55(1):52-66. doi: 10.1111/cea.14592, PMID 39506931.
Jain D. Clinico-epidemiological and radiological study of chronic rhinosinusitis in Western Maharashtra. Indian J Appl Res. 2017;7(4):145-6.
Gardner WJ. The control of bleeding during an operation by induced hypotension. J Am Med Assoc. 1946 Nov 9;132(10):572-4. doi: 10.1001/jama.1946.02870450026007, PMID 21001599.
Noori F, Emami MR, Nakhaee P, Mohri M. Comparison of two anesthetic inhalant agents (isoflurane and sevoflurane) on induction and recovery from anesthesia physiological effects hematocrit and biochemistry profiles in domestic pigeons (Columba livia domestica). J Poult Sci Avian Dis. 2023;1(2):18-27. doi: 10.61838/kman.jpsad.1.2.3.
Eger EI. The pharmacology of isoflurane. Br J Anaesth. 1984;56 Suppl 1:71S-99S. PMID 6391530.
De Hert S, Moerman A. Sevoflurane. F1000Res. 2015 Aug 25;4:626. doi: 10.12688/f1000research.6288.1, PMID 26380072.
Ozkiris M, Kapusuz Z, Ozturk S, Bolat E, Saydam L. The effects of sevoflurane and isoflurane in nasal septal surgery. J Craniofac Surg. 2013 Mar;24(2):592-5. doi: 10.1097/SCS.0b013e3182802029, PMID 23524751.
Ahsan B, Masaeli M, Majedi MA, Ghaderi E, Faraji T. Maintenance of anesthesia in paranasal endoscopic sinus surgery: sevoflurane or isoflurane? Which one is better? J Clin Res Paramed Sci. 2022;11(1):e122247. doi: 10.5812/jcrps-122247.
Sivaci R, Yilmaz MD, Balci C, Erincler T, Unlu H. Comparison of propofol and sevoflurane anesthesia by means of blood loss during endoscopic sinus surgery. Saudi Med J. 2004 Dec;25(12):1995-8. PMID 15711683.
Cantillo J, Goldberg ME, Larijani GE, Vekeman D. Recovery parameters after sevoflurane and isoflurane anesthesia. Pharmacotherapy. 1997 Jul-Aug;17(4):779-82. doi: 10.1002/j.1875-9114.1997.tb03755.x, PMID 9250557.