
Int J Curr Pharm Res, Vol 17, Issue 6, 143-145Case Study
INCIDENTAL DETECTION OF PRIMARY STRUMAL CARCINOID TUMOR IN A NORMAL SIZE OVARY: A RARE CASE REPORT WITH AVAILABLE REVIEW OF LITERATURE
PRAGNYA PARAMITA MISHRA1, PREMANAND PANDA2*
1Department of Pathology, Hi-Tech MCH, Rourkela, Odisha, India. 2Department of Radiology, JP Hospital and Research Centre, Rourkela, Odisha, India
*Corresponding author: Premanand Panda; *Email: panda.premanand@gmail.com
Received: 15 Aug 2025, Revised and Accepted: 05 Oct 2025
ABSTRACT
Struma ovarii is an extremely rare type of malignant germ cell tumor and its incidence is 0.1% of all ovarian malignancies. Only 5 percent of carcinoid cancers originate in the ovary. The histopathology is a combination of carcinoid and thyroid tissue along with other components of mature teratoma. In this case, patient was presented with irregular menses only. No ovary related symptoms were seen. We are
Keywords: Primary strumal carcinoid tumor, Ovary
© 2025 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2025v17i6.7067 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Struma ovarii is an extremely rare type of malignant germ cell tumor. Its incidence is 0.1% of all ovarian malignancies [1]. The histological character is a combination of carcinoid and normal thyroid tissue. Primary ovarian carcinoids are extremely rare. Most cases are reported in perimenopausal ages. Only 5 percent of carcinoid cancers originate in the ovary [1]. Patients with strumal carcinoid rarely exhibit the typical signs of carcinoid syndrome. Instead, the tumor is occasionally discovered by accident, and patients may have symptoms like abdominal distension that are brought on by the size of the tumor. The four different histologic patterns of arrangement of cells in carcinoids are mucinous, strumal, trabecular, and insular. As metastasis is extremely rare, simple oophorectomy or salpingo-oophorectomy is sufficient for survival. Here, we describe a 48-year-old woman who had an unintentionally detected strumal carcinoid with a focal rhabdomyosarcoma-like region.
CASE REPORT
A 48 y old female presented with the complaint of irregular menses for the last 6 mo. The patient came to visit the gynecology OPD. The patient underwent abdominal and pelvic ultrasonography, which showed a subserosal fibroid and a normal-sized right ovary with an internal echogenic focus. Bilateral fallopian tubes and the other ovary were unremarkable. No free fluid was found on ultrasonography. The contrast CT scan shows (fig. 1) a normal-sized right ovary with a fat attenuation lesion and internal eccentric calcification. Routine blood hemogram along with thyroid and heart examination, were normal. On physical examination, no organomegaly was found.
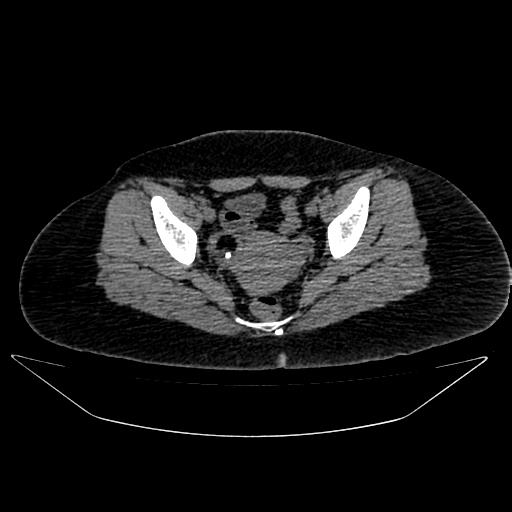
Fig. 1: Normal-sized right ovary with a fat attenuation lesion and internal eccentric calcification
Due to a preoperative diagnosis of fibroid, the patient underwent bilateral salpingo-oophorectomy and total abdominal hysterectomy. A normal-sized uterus with a subserosal fibroid was discovered during surgery. The bilateral fallopian tube, left ovary, and other viscera of the abdomen were within normal limits. Histopathology showed the cervix measured 3.0 × 2.5 × 2.0 cm and the uterus measured 10.0 × 6.0 × 4.0 cm. The thickness of the myometrium and endometrium were 1.5 cm and 0.4 cm, respectively. The right ovary measures 4.0 x 3.5 x 3.0 cm, is diffusely lobulated, and has a smooth exterior (fig. 2).
Fig. 2: Right ovary measures 4.0 x 3.5 x 3.0 cm, is diffusely lobulated, and has a smooth exterior
The cut surface is solid-cystic, and show two distinct tumours. (fig. 3) The cysts were filled with mucus. A firm, homogenous, 3.1 cm-diameter, tan-brown to yellow nodule was seen. The cut surface was unremarkable.

Fig. 3a: Cut surface is solid-cystic, and shows two distinct tumours
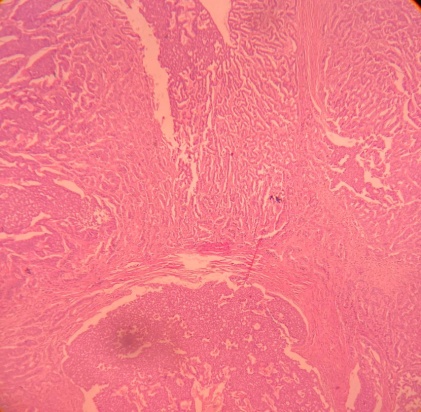
Fig. 3b: Microscopy shows two distinct tumours
The histopathology section from the right ovary shows a cyst walled by stratified squamous epithelium with skin appendages, hair follicles, mature cartilage, and fat tissue. Thyroid tissue and colloid-filled thyroid follicles made up a portion of the solid nodule (fig. 4)
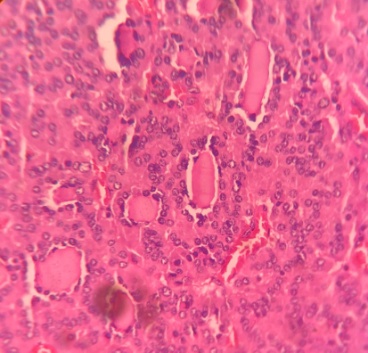
Fig. 4: Thyroid tissue and colloid-filled thyroid follicles
A tumor cell with sheets of monomorphic cells (fig. 5) with copious amounts of granular cytoplasm organized in nests and an insular pattern was also observed. There is scattered mitosis. The nuclear chromatin had a "salt and pepper" look and was finely granular.
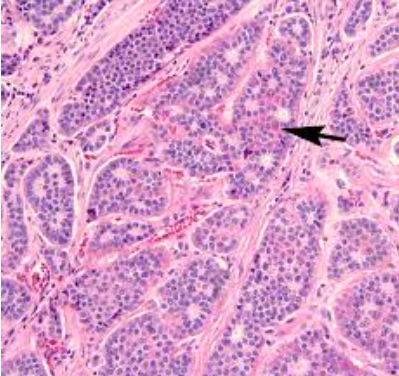
Fig. 5: Sheets of monomorphic cells organized in nests and an insular pattern
Rhabdomyoblast-like cells were visible at a tiny microscopic focus (fig. 6). Based on the histopathology, strumal carcinoid with a small number of rhabdomyoblast-like cells was diagnosed.
Blocks were subjected to immunohistochemical analysis of the patient, which revealed that while the follicular structure tested positive for TTF, the cord and insular sequences tested positive for synaptophysin and chromogranin. The histopathological diagnosis was supported by the rhabdomyoblastic cells' desmin positivity.
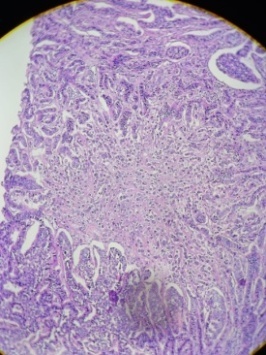
Fig. 6: Rhabdomyoblast-like cells in tiny focus
There was no evidence of tumor rupture during surgery. No intra-abdominal adhesions, including those surrounding the tumor, were seen. The patient had a favorable postoperative course, and on the ninth postoperative day, she was released from the hospital without any problems. There were no deposits in the omentum, uterus, or adnexa, and there was no evidence of lymph node metastases. Ascites cytology also came up negative. The patient was diagnosed as ovarian strumal carcinoid, stage IA, pT1aN0M0, based on these findings. No sign of recurrence has been seen to date. Additionally, the patient's tumor indicators were continuously monitored.
DISCUSSION
Carcinoids are tumors that resemble neuroendocrine tumors of grade 1. Clinically, it is primarily unilateral and occurs in both young and old women [1]. Furthermore, they can appear as masses or nodules in ovarian struma, mature teratoma, and, less frequently, mucinous cystadenoma. [1] Constipation [2] may accompany carcinoid tumors that produce peptide YY. According to the WHO classification (2020), carcinoid tumors are categorized as "monodermal teratomas and somatic-type tumors arising from dermoid cysts. Scully originally characterized ovarian strumal carcinoid in 1970 [3]. It is a very uncommon tumor, occurring in less than 0.1% of all ovarian malignant tumors, according to reports. [4] Furthermore, strumal carcinoids comprise 21.9% of ovarian carcinoids, and ovarian carcinoids [5] account for 0.1% of all ovarian malignant tumors. A tumor unique to the ovary, strumal carcinoid has combined histological characteristics of both struma and carcinoid components.
Clinical manifestations of carcinoids may include heart problems, diarrhea, bloating in the abdomen, and flushing of the face. Prostaglandin [6], tachykinin, bradykinin, kallikrein, substance P, histamine, and serotonin are all produced and secreted by tumors. Strum carcinoid, on the other hand, rarely shows conventional symptoms or test results and is frequently found by lower abdomen inspection. According to Robboy and Scully [7] a rise in steroid hormone was noted in about 8% of instances in terms of endocrine function.
Rhabdomyoblastis differentiation is extremely rare in the ovary; however, a few cases are reported in the testis [8]. However, in our case, a very focal area was showing rhabdomyoblast-like cells, which were showing moderate desmin positivity.
CONCLUSION
Most patients have benign strumal carcinoid, and oophorectomy or salpingo-oophorectomy is a successful treatment. Proper grossing with multiple serial sectioning and serology will be helpful in identifying other associated minor components and thereby helping in proper management.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCES
WHO. Classification of Tumours Editorial Board, 5th edition: Female Genital Tumours WHO Classification of Tumours Editorial Board Lyon; 2020. p. 132-5.
Motoyama T, Katayama Y, Watanabe H, Okazaki E, Shibuya H. Functioning ovarian carcinoids induce severe constipation. Cancer. 1992 Jul 15;70(2):513-8. doi: 10.1002/1097-0142(19920715)70:2<513::aid-cncr2820700223>3.0.co;2-p, PMID 1617602.
Scully RE. Recent progress in ovarian cancer. Hum Pathol. 1970;1(1):73-98. doi: 10.1016/s0046-8177(70)80005-3, PMID 4330995.
Kanasugi M, Nishiyama H, Sanpei M, Asano S, Honda T. Ovarian strumal carcinoid: a case report. Fukushima J Med Sci. 2023 Apr 5;69(1):51-5. doi: 10.5387/fms.2022-22, PMID 36878591.
Lenicek T, Tomas D, Soljacic Vranes H, Kraljevic Z, Klaric P, Kos M. Strumal carcinoid of the ovary: report of two cases. Acta Clin Croat. 2012 Dec;51(4):649-53. PMID 23540174.
Sharma R, Biswas B, Wahal S, Sharma N, Kaushal V. Primary ovarian carcinoid in mature cystic teratoma: a rare entity. Clin Cancer Investig J. 2014;4(1):80-2. doi: 10.4103/2278-0513.125803.
Robboy SJ, Scully RE. Strumal carcinoid of the ovary: an analysis of 50 cases of a distinctive tumor composed of thyroid tissue and carcinoid. Cancer. 1980;46(9):2019-34. doi: 10.1002/1097-0142(19801101)46:9<2019::aid-cncr2820460921>3.0.co;2-w, PMID 7427909.
Lovric E, Hizak DB, Balja MP, Lenicek T, Kruslin B. An unusual mixed germ cell tumor of the testis consisting of rhabdomyosarcoma mature teratoma and yolk sac tumor. Asian J Androl. 2010 May;12(3):451-2. doi: 10.1038/aja.2010.2, PMID 20173766.