
Int J Curr Pharm Res, Vol 18, Issue 2, 48-56Original Article
AN OBSERVATIONAL STUDY ON EMPIRICAL THERAPY IN ICU PATIENTS WITH SEPSIS IN A TERTIARY CARE HOSPITAL
A. R. SHABARAYA, MINCHU ARUNKUMAR SUNKADAKATTE*, JESSICA MARYIOLA FERNANDES, CHANDANNA K. ADIYODI, MUHAMMED SHAMIL N. P., SUDHAMSHU K. TANTRY
Department of Pharmacy Practice, Srinivas College of Pharmacy, Valachil, Post Farangipete, Mangalore-574143, Karnataka, India
*Corresponding author: Minchu Arunkumar Sunkadakatte; *Email: minchuas2@gmail.com
Received: 14 Nov 2025, Revised and Accepted: 01 Jan 2026
ABSTRACT
Objective: Sepsis is a life-threatening organ dysfunction caused by dysregulated host response to an infection. This study investigated antibiotic prescribing patterns, antimicrobial resistance, and their impact on prognosis and quality of life in critically ill patients with sepsis.
Methods: A prospective observational study was conducted at Srinivas Institute of Medical Science and Research Centre. For over six months, 174 ICU patients diagnosed with sepsis were assessed. Patient demographics, infection source, Sequential Organ Failure Assessment (SOFA) scores, antibiotic regimens, and clinical outcomes were collected.
Results: The study population was predominantly male (69.54%) with a mean age of 54 y. Piperacillin/Tazobactam (46.55%) and Meropenem (36.78%), both classified as WHO Watch antibiotics of AWaRe Classifications, were the most commonly prescribed antibiotics. This suggests a potential deviation from WHO guidelines and raises concerns about antibiotic resistance. Pseudomonas (15%) was the leading pathogen, exhibiting high resistance levels. While SOFA scores did not significantly differ between survivors and non-survivors, they correlated with length of stay, indicating disease severity. The SF-20 questionnaire revealed poor health perception and reduced social functioning across all age groups in surviving patients, impacting quality of life.
Conclusion: This study highlights a trend of over-prescription of broad-spectrum antibiotics, potentially deviating from WHO recommendations. The dominance of highly resistant g-negative bacteria underscores the need for targeted antibiotic selection based on local resistance patterns. SOFA scores reflected disease severity but did not predict mortality. The study emphasizes the lasting impact of sepsis on patients' physical, social, and mental well-being, suggesting the importance of comprehensive post-discharge rehabilitation programs.
Keywords: Sepsis, Empirical Antibiotics, SOFA, AWaRe classifications, Critical care
© 2026 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2026v18i2.8057 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Sepsis is defined as a “life-threatening organ dysfunction caused by a dysregulated host response to an infection”, where organ dysfunction is identified when there is a sudden rise of two or more points in the total Sequential Organ Failure Assessment (SOFA) score, attributed to an infection [1]. Empirical antibiotic treatment provides a better outcome with its prompt therapy initiation. Drugs, under this category are most commonly prescribed among patients in ICU primarily to treat contamination and colonization [2]. The excessive use of broad-spectrum antibiotics in critically ill patients, even in the absence of resistance risk factors, can elevate the likelihood of resistance development.
The WHO addresses antibiotic issues through the AWaRe Classification, categorizing them as Access, Watch, and Reserve. Access involves common infection treatments, Watch has a higher resistance risk, and Reserve is encouraged as a last resort [3]. The WHO 13th General Programme of Work 2019-2023 has initiated a country-level target of at least 60% of total antibiotic consumption being from Access group antibiotics [4]. Global antibiotic consumption has been on a steady rise alongside the emergence of antibiotic resistance, dampening effective treatment [6]. The epidemiology of sepsis, encompassing its causes, prevalence, and outcomes, varies across regions. Approximately 48.9 million people are affected by sepsis annually, leading to an estimated 11 million deaths, which accounts for up to 19.7% of the global mortality rate [7]. The Global Burden of Disease Study provided an indirect estimate that India has approximately 11 million sepsis cases, resulting in nearly 3 million deaths [8].
Overall, 75% of individuals who survive sepsis experience at least one new medical, psychological, or cognitive condition following their hospital discharge. Those who survive sepsis undergo a decline in health-related quality of life (HRQoL), especially in the physical domain, which persists for at least five years after discharge. Numerous sepsis survivors contend with both physical and cognitive impairments [5]. Sepsis, being a life-threatening condition requires immediate treatment (within an hour of admission), and its management is composed of 6Rs, namely, right patient, right time, right target, right antibiotics, right dose, and right source control [3]. Therefore, this study enabled categorizing the antibiotics used in ICU, whilst referring the prescribing pattern to the AWaRe Classification and determining the SOFA scoring system, along SF20 questionnaire to understand the health-related quality of life post sepsis, as sepsis survival patients exhibit poor physical and/or psychological effects.
MATERIALS AND METHODS
Study design and participants
A prospective, observational study was carried out on empirical therapy in Srinivas Institute of Medical Sciences and Research Centre, Mukka, Mangalore on ICU patients with sepsis between March 2024 and August 2024. The inclusion criteria involved patients aged 18y and above, provided that they were admitted to the ICU, diagnosed with sepsis and post-discharge sepsis survivors. Pregnant women were excluded from the study.
Operational modality
Data collection form included the patient’s demographic details, co-morbid diseases, past history of medical condition, medication history, laboratory details, site of infection, site-specific culture test, final diagnosis, empirical and definite treatment chart. It also includes SOFA scoring chart to assess patient status within 24 h of admission and SF 20 questionnaire for sepsis survivors post discharge. Ethical Clearance was obtained and the patients for the study were selected based on the inclusion and exclusion criteria. During the hospital visit, we explained the study participants about the study and obtained the consent for collecting data. During the course of 6 mo of study, required data was collected from the medical records and the data collected was analyzed according to the objectives made in this study.
Statistical analysis
Statistical analysis involves collecting and scrutinizing all data sample in a set of items from which samples can be drawn and a suitable statistical test was applied to analyze the data. The collected data was analyzed using Microsoft Excel.
RESULTS
Characteristics of study subjects
A total of 174 ICU patients diagnosed with sepsis were included in the study, out of which 121 (69.54%) were males. The mean age of patients was 54.09±16.14 y (mean±SD). The patients aged between 55-64 y had higher prevalence of sepsis followed by 45-54 y of age group i. e., 22.99% and 19.54% respectively.
Out of 174 patients, 147 had LOS>3 d and the remaining had ≤3 d. Of the patients, 44 (25.29%) required ventilation, while 130 (74.71%) did not require ventilation. The majority of the patients, 136 (78.16%), had a SOFA score of less than 8, while 38 (21.84%) had a score of 8 or higher. The Total Leukocyte Count (TLC) distribution shows that 10 patients (5.75%) had a count of less than 4000, 78 patients (44.82%) had a count between 4000 and 11000 cells/mm3, and 86 patients (49.43%) had a count exceeding 11000 cells/mm3. The major source of infection was respiratory infections (35.05%) followed by source unidentified (29.31%), skin and soft tissue infections (18.40%), urinary tract infection (13.80%) and other infections (3.44%), which includes medical device-associated infections fig. 1.
Among the patients, 75 (43.10%) had two or more co-morbidities, 70 (40.23%) had less than two co-morbidities, and 29 (16.67%) had no co-morbidities. The outcome distribution revealed that 136 patients (78.16%) survived, 16 patients (9.2%) did not survive, and 22 patients (12.64%) had an unknown outcome. Shown in table 1.
Table 1: Characteristics of the study subjects (N=174)
| Characteristics | Frequency | Percentage |
Age in years
|
8 16 24 34 40 33 19 |
4.61% 9.19% 13.79% 19.54% 22.99% 18.96% 10.92% |
Gender
|
121 53 |
69.54% 30.46% |
Length of stay in days (LOS)
|
27 147 |
15.52% 84.48% |
Ventilation use
|
44 130 |
25.29% 74.71% |
Total Leukocyte Count (cells/mm3)
|
10 78 86 |
5.75% 44.82% 49.43% |
Source of infection
|
61 51 32 24 6 |
35.05% 29.31% 18.40% 13.80% 3.44% |
Number of Co-morbidities
|
75 70 29 |
43.10% 40.23% 16.67% |
Clinical outcome
|
136 16 22 |
78.16% 9.20% 12.64% |
Relation between various sources of infection and different age groups
Table 2 shows the association between various sources of infection among different age groups analyzed using the chi-square test. The test revealed that there is no significant association between various sources of infection and different age groups, indicating that age does not influence source of infection (p-value =>0.05).
Relation between age and length of stay (LOS)
Table 3 represents, Pearson correlation analysis performed to examine the relationship between age and LOS. The results showed that there is no significant correlation between the two variables, indicating that the age does not have a significant influence on the length of stay in the ICU. (p-value =>0.05).
Empirical prescribing pattern according to WHO AWaRe classification
A total of 174 patients with sepsis were screened during the study period in the tertiary care hospital and the empirical antibiotics administered to them were assessed accordingly. A list of antibiotics was sorted out initially to determine the most prescribed category of antibiotic in the hospital. Table 4 represents, the names of all the empirical antibiotics administered to the patients included in the study, along with their antibiotic class and number of drugs.
Beta lactam/beta lactamase inhibitor (83) was a highly used empirical antibiotic category, for numerous sepsis cases in the hospital, which was either continued as definitive therapy or switched to another antibiotic post-culture sensitivity. This brings attention towards the extensive utilization of broad-spectrum antibiotics in disease treatment and management.
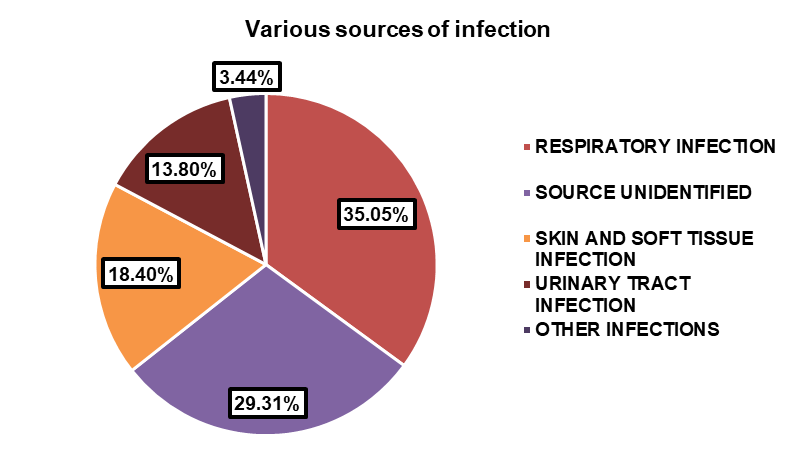
Fig. 1: Various sources of infection
Table 2: Relation between different age groups and various sources of infections
| Source of infection | Respiratory infection | Source unidentified | Skin and soft tissue infection |
Urinary tract infection | Other infection | Total |
| Age group | ||||||
| 18 – 24 | 1 | 1 | 2 | 4 | 0 | 8 |
| 25 – 34 | 4 | 10 | 0 | 2 | 0 | 16 |
| 35 – 44 | 7 | 7 | 6 | 3 | 1 | 24 |
| 45 – 54 | 12 | 13 | 5 | 3 | 1 | 34 |
| 55-64 | 19 | 7 | 9 | 4 | 1 | 40 |
| 65 – 74 | 11 | 8 | 5 | 7 | 2 | 33 |
| 75-84 | 7 | 5 | 5 | 1 | 1 | 19 |
| Total | 61 | 51 | 32 | 24 | 6 | 174 |
| p-value | >0.05 |
Table 3: Relation between age and LOS
| Variable | p-value | Significance |
| Age (overall) | >0.05 | The association between age and LOS is NOT Statistically significant. |
| LOS (overall) |
Table 4: Data collected on empirical antibiotics administered
| Antibiotics | Category of antibiotic | Frequency |
| Piperacillin/Tazobactam | Beta lactam/beta lactamase inhibitor | 81 |
| Meropenem | Carbapenems | 64 |
| Ceftriaxone | Third gen cephalosporin | 17 |
| Linezolid | Oxazolidinones | 14 |
| Metronidazole | Imidazole | 14 |
| Azithromycin | Macrolide | 11 |
| Cefoperazone/Sulbactam | Second gen cephalosporin | 7 |
| Rifaximin | Rifamycin | 6 |
| Clindamycin | Lacosamide | 5 |
| Cefotaxime | Third gen cephalosporin | 5 |
| Doxycycline | Tetracycline | 4 |
| Tigecycline | Glycylcyclines | 3 |
| Cefuroxime | Second gen cephalosporin | 2 |
| Amikacin | Aminoglycosides | 2 |
| Amoxicillin/clavulanic acid | Beta lactam/beta lactamase inhibitor | 2 |
| Faropenem | Penems | 2 |
| Piperacillin | Penicillin | 1 |
| Vancomycin | Glycopeptides | 1 |
The data presented in this table illustrates that medications categorized under the Watch group (81%) were the most frequently administered, with Piperacillin/Tazobactam (46.55%) emerging as the predominant empirical antibiotic prescribed, likely due to its broad-spectrum characteristics. Following closely behind were Meropenem (36.78%) and Ceftriaxone (9.77%), both falling within the same classification.
In contrast, the utilization of drugs categorized under the Access group (11%) was moderate in comparison to the Watch class in empirical therapy. Metronidazole (8.05%) emerged as the foremost drug within this category. Furthermore, drugs categorized under the Reserve group (8%) were the least utilized during the study period. The AWaRe class distribution is figuratively represented in fig. 2.
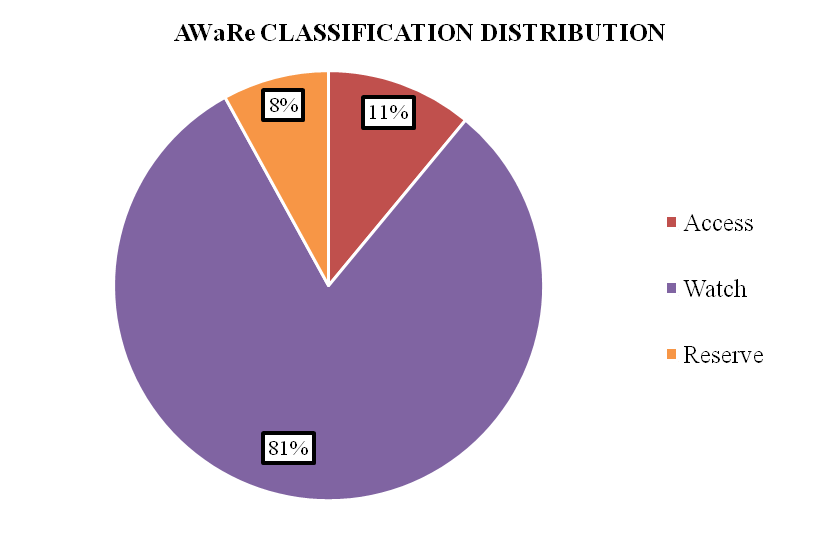
Fig. 2: Distribution of access, watch and reserve category drugs in the prescribing
Fig. 3, provides an insightful depiction of the prescription patterns, specifically focusing on the number of antibiotics administered as empirical therapy, clinical practices surrounding antibiotic usage, shedding light on the trends and preferences within the healthcare setting. Monotherapy within the Watch class exhibited a higher frequency of utilization compared to other classes. Similarly, combination therapy involving two drugs showed a comparable pattern. This trend was followed by drugs given in combination of two, belonging to Access+Watch and Watch+Reserve classes, respectively. Reserve drugs were the least utilized, both in combination therapy and monotherapy.
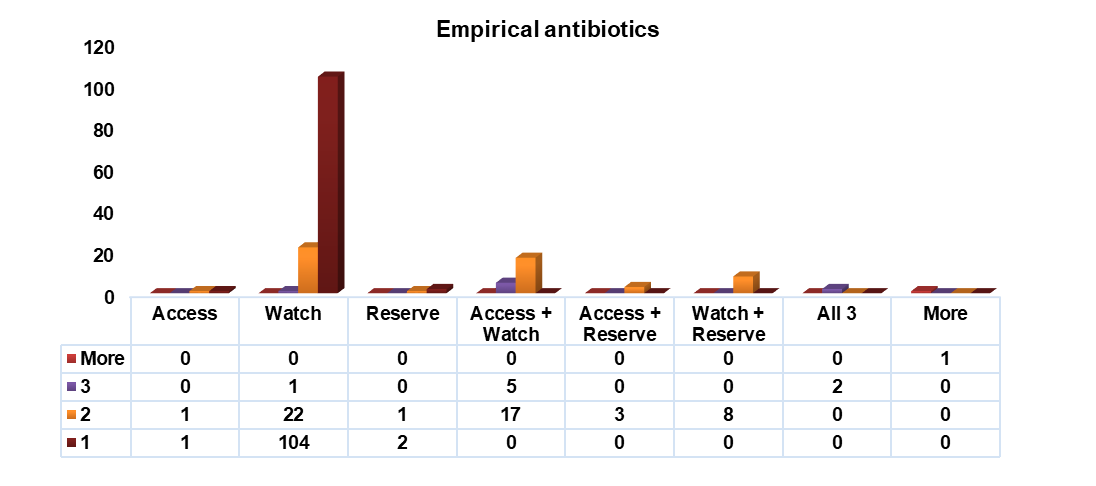
Fig. 3: Description of empirical antibiotics administered
Pattern of microbial culture
Based on the results of bacterial cultures, g negative bacteria were more predominant than g positive bacteria. 48 cultures showed no growth from various specimens while mixed/multiple growth and fungal growth was found to be in 7 and 7 subjects, respectively. Mixed/multiple growth are the cultures where two different specimens have different bacteria isolated in same person or any one specimen having more than one bacterial growth. In g negative organisms, Pseudomonas aeruginosa (15%) was found to be prevalent followed by Klebsiella pneumoniae (14%), Escherichia. coli (13%) and Acinetobacter baumannii (8%). Coagulase negative staphylococcus was found to be prevalent in g positive organisms, shown in table 5.
Resistance to commonly prescribed empirical drugs
The most commonly prescribed empirical drugs were Piperacillin/Tazobactam, Meropenem, Ceftriaxone, Linezolid, Metronidazole, Azithromycin, Cefoperazone/Sulbactam. According to the resistance pattern of cultures, K. pneumoniae was found to have resistance to all the empirical antibiotics prescribed except Linezolid, whereas Coagulase negative staphylococcus showed resistance to Linezolid and Cefoperazone/Sulbactam fig. 4 and 5 shows, the resistance profile of g negative and g-positive organisms to commonly prescribed empirical drugs, respectively.
Table 5: Different species isolated from various specimens
| Species | n (%) | Specimens |
| Gram-negative organisms | ||
| Klebsiella pneumoniae | 26 (14) | Sputum, Urine, Pus, Blood |
| Escherichia coli | 22 (13) | Pus, urine |
| Pseudomonas aeruginosa | 27 (15) | Sputum, urine, blood, pus, catheter tip |
| Acinetobacter baumannii | 15 (8) | Sputum, pus, urine, suction tip, ET tube |
| Proteus mirabilis | 1 (1) | Pus |
| Gram-positive organisms | ||
| MSSA | 3 (2) | Pus |
Coagulase negative Staphylococcus (CoNS) |
9 (5) | Pus, blood, urine |
| Proteus vulgaris | 1 (1) | Pus |
| MRSA | 1(1) | Pus |
| Enterococcus faecalis | 4 (3) | Pus, urine |
| Enterobacter species | 3 (2) | Urine, blood |
| Mixed growth/Multiple growth | 7 (4) | Sputum, urine |
| No growth | 48 (27) | Pus, urine, sputum |
| Fungal growth | 7 (4) | Urine, sputum, vaginal swab |
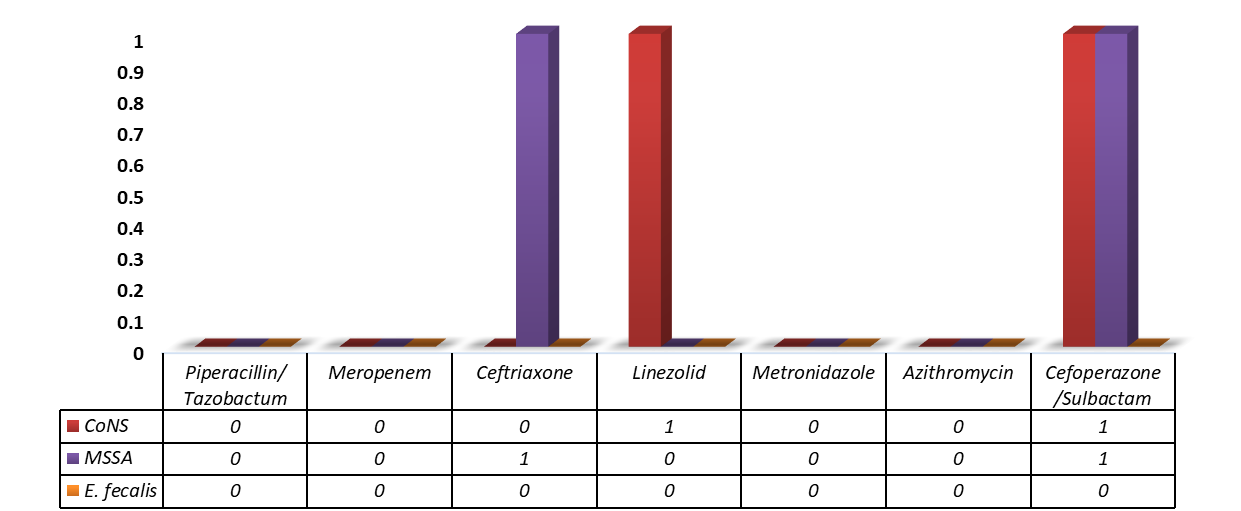
Fig. 4: Antimicrobial resistance profile of g-negative organisms for commonly prescribed empirical drugs
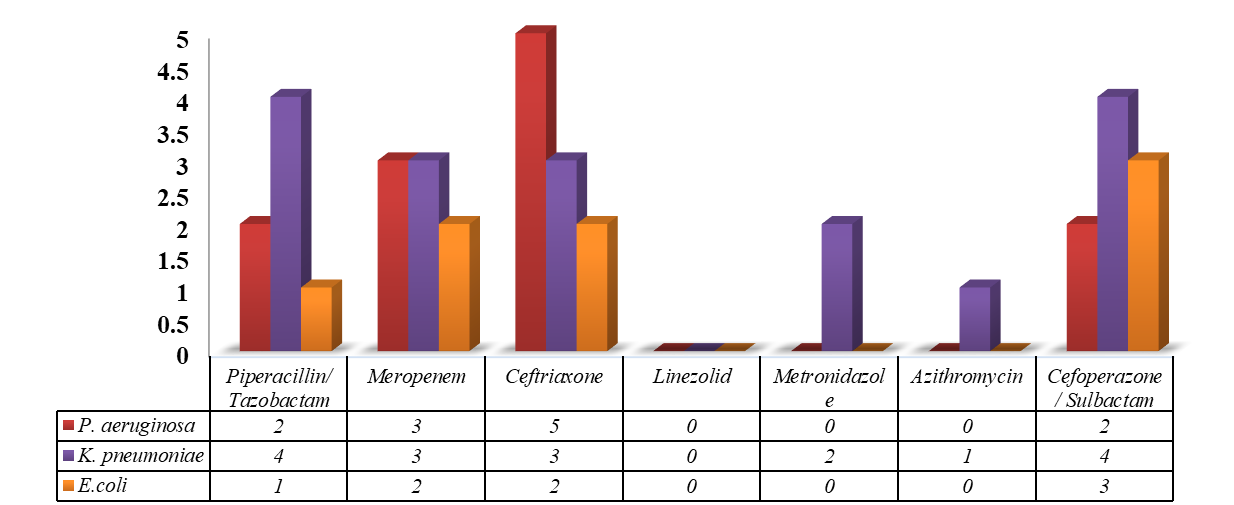
Fig. 5: Antimicrobial resistance profile of g-positive organisms for commonly prescribed empirical drug
Table 6 represents the association of age groups with most prevalent bacteria. The association was carried out using chi-square test and it revealed that there is significant association between different age groups and various prevalent bacteria (p-value =<0.05).
Predicting the prognosis of patients with sepsis using SOFA scores
Among 174 patients screened, 40 patients were excluded from the study, in which 18 patients had two or more missing data while 22 patients went against medical advice. The non-survivors were 15 among 134 patients whose SOFA score was calculated. The admission SOFA score ranged from 2 to 14. The highest SOFA score among the non–survivors was found to be 12. The length of stay varied, independent to mortality.
The relation of admission SOFA score and length of stay (LOS) is depicted in the form of unpaired T statistics in table 8.
Table 6: Age in relation to bacterial growth
| Age group | Pseudomonas aeruginosa | Klebsiella pneumoniae | E. coli |
Acinetobacter baumannii | Coagulase negative staphylococcus | Total |
| 18 – 24 | 1 | 0 | 1 | 0 | 1 | 6 |
| 25 – 34 | 0 | 4 | 2 | 0 | 1 | 5 |
| 35 – 44 | 5 | 5 | 4 | 1 | 0 | 11 |
| 45 – 54 | 8 | 7 | 3 | 1 | 2 | 24 |
| 55 – 64 | 5 | 2 | 8 | 5 | 4 | 25 |
| 65 – 74 | 5 | 5 | 1 | 7 | 1 | 18 |
| 75 – 84 | 3 | 3 | 3 | 1 | 0 | 10 |
| Total | 27 | 26 | 22 | 15 | 9 | 99 |
| p-value | <0.05 |
Table 7, depicts the chi-square test conducted to analyze the association between WHO AWaRe category of empirical therapy and type of bacteria i. e., g negative bacteria, g positive bacteria and mixed/multiple growth. The test revealed that there exists a highly significant association between the two variables (p-value = <0.001).
Table 7: Relation between type of bacterial growth and empirical therapy
| Type of organisms Empirical therapy | Gram-negative bacteria | Gram-positive bacteria | Mixed/multiple growth | Total |
| Access | 2 | 0 | 0 | 2 |
| Watch | 68 | 6 | 4 | 78 |
| Reserve | 3 | 0 | 0 | 3 |
| Access+Watch | 13 | 9 | 0 | 22 |
| Access+Reserve | 2 | 0 | 1 | 3 |
| Watch+Reserve | 7 | 1 | 0 | 8 |
| Access+Watch+Reserve | 1 | 0 | 1 | 2 |
| More | 0 | 0 | 1 | 1 |
| Total | 96 | 16 | 7 | 119 |
| p value | <0.001 |
Table 8: The relation of admission SOFA score and length of stay (LOS) with clinical outcome
| LOS | SOFA | |
| Mean±Standard deviation among all patients | 5.91±2.84 d | 8.26±4.7 d |
| Mean±Standard deviation among all survivors | 8.37±4.15 d | 5.80±2.82 d |
| Mean±Standard deviation among all non-survivors | 7.33±8.32 d | 6.73±2.78 d |
| p-value | >0.05 | >0.05 |
The mean length of stay (LOS) among all patients was found to be 5.91 d with a standard deviation of 2.84 d, while the mean Sequential Organ Failure Assessment (SOFA) score was 8.26 with a standard deviation of 4.7 d. Among survivors, the mean LOS increased to 8.37 d, with a standard deviation of 4.15 d, whereas the mean SOFA score decreased to 5.80 d, with a standard deviation of 2.82 d. Conversely, non-survivors exhibited a mean LOS of 7.33 d with a standard deviation of 8.32 d, and a mean SOFA score of 6.73 d with a standard deviation of 2.78 d.
Based on the study results, there was no statistically significant difference observed in the mean LOS between survivors and non-survivors (p-value =>0.05). Similarly, there was no statistically significant difference observed in the mean SOFA score between survivors and non-survivors (p-value =>0.5).
The correlation between SOFA Scores and LOS is depicted in the form of Spearman correlation coefficient statistics, shown in table 9.
The Spearman correlation statistical analysis demonstrated a p-value of<0.01, indicating a statistically significant association between the SOFA score and length of stay (LOS). This indicates a positive correlation between admission SOFA score and LOS, i. e., as the SOFA score increases; the LOS also tends to increase. However, the correlation is not strong, as the value is relatively low. A rho value of 1 indicates a perfect positive correlation; while-1 indicate a perfect negative correlation.
The correlation between SOFA score and clinical outcome is depicted in the form of Point Bi-Serial correlation coefficient statistics as shown in table 10.
Table 9: Correlation between SOFA Score and LOS
| Variable | p-value | Significance |
| SOFA score (overall) | <0.01 | The association between SOFA score and LOS is statistically significant. |
| LOS (overall) |
Table 10: Correlation between SOFA score and clinical outcome
| Variable | p-value | Significance |
| SOFA Score (overall) | >0.05 | The association between SOFA Score and Clinical outcome is statistically NOT significant |
| Clinical outcome (overall) |
The point biserial correlation analysis revealed a p-value of<0.05. This indicates a weak negative correlation between SOFA scores and clinical outcome i. e., higher SOFA scores are associated with slightly lower likelihood of a positive clinical outcome. The correlation coefficient is relatively close to 0, indicating a weak correlation between two variables. This signifies the two variables are statistically not significant.
Table 11 represents chi-square analysis between SOFA scores and various age groups. The results showed that there is no significant association between two variables.
Table 11: Association of SOFA score with age
| Age groups | SOFA scores | Total | |
| SOFA score <8 | SOFA score ≥8 | ||
| 18 – 24 | 3 | 2 | 5 |
| 25 – 34 | 6 | 3 | 9 |
| 35 – 44 | 12 | 5 | 17 |
| 45 – 54 | 14 | 14 | 28 |
| 55 – 64 | 22 | 9 | 31 |
| 65 – 74 | 24 | 3 | 27 |
| 75-84 | 14 | 3 | 17 |
| Total | 95 | 39 | 134 |
| p-value | >0.05 |
Table 12 shows the association between SOFA scores and gender (male and female) analyzed by using T test. The mean±SD among males was found to be 5.92±2.81 and females 6.06±2.85. The test revealed no statistical significance in SOFA scores between males and females (p-value =>0.05).
Table 12: Relation between SFOA scores and gender
| SOFA scores | |
| Mean±Standard deviation among all patients | 8.26±4.7 |
| Mean±Standard deviation among all males | 5.92±2.81 |
| Mean±Standard deviation among all females | 6.06±2.85 |
| p-value | >0.05 |
Evaluating the health-related quality of life in sepsis survivors using SF-20
On further analysis of our study involved sepsis survivors whose SOFA scores were calculated. Among 134 patients, 15 of them did not survive during the hospital stay, 8 patients did not survive post-discharge while 5 of them did not participate in the HRQoL survey. The SF 20 questionnaire consists of 6 domains namely, Health perception (Q1, 12a, 12b, 12c, 12d), Bodily pain (Q3), Physical functioning (Q2a, 2b, 2c, 2d, 2e, 2f), Role functioning (Q4 and 5), Social functioning (Q6) and Mental health (Q7, 8, 9, 10, 11).
Table 13: Correlation of various variables with domains of SF 20
| Variable | Health perception | Bodily pain | Physical functioning | Role functioning | Social functioning | Mental health | |
| Age | |||||||
| 18 – 24 | Mean | 49.11 | 48.13 | 56.08 | 57.29 | 42.71 | 56.37 |
| SD | 26.11 | 23.50 | 34.98 | 35.43 | 26.54 | 22.53 | |
| 25 – 34 | Mean | 50.57 | 47.17 | 66.51 | 65.09 | 39.25 | 55.89 |
| SD | 26.82 | 23.24 | 34.89 | 36.63 | 28.81 | 23.22 | |
| 35 – 44 | Mean | 48.96 | 49.31 | 54.62 | 56.44 | 41.78 | 56.50 |
| SD | 26.17 | 23.42 | 34.90 | 35.03 | 26.24 | 22.39 | |
| 45 – 54 | Mean | 49.05 | 48.63 | 56.23 | 58.42 | 41.47 | 56.40 |
| SD | 26.07 | 23.64 | 34.58 | 34.45 | 26.62 | 22.56 | |
| 55 – 64 | Mean | 48.99 | 49.04 | 54.97 | 56.25 | 42.12 | 56.40 |
| SD | 26.06 | 23.30 | 34.80 | 34.53 | 26.28 | 22.37 | |
| 65-74 | Mean | 48.92 | 49.28 | 55.33 | 57.22 | 41.44 | 56.47 |
| SD | 26.21 | 23.82 | 34.80 | 35.26 | 26.34 | 22.51 | |
| 75-84 | Mean | 48.87 | 49.22 | 54.82 | 55.88 | 42.55 | 56.37 |
| SD | 26.36 | 23.66 | 35.11 | 35.30 | 26.35 | 22.47 | |
| p-value | >0.05 | >0.05 | <0.01* | <0.05* | >0.05 | >0.05 | |
| Gender | |||||||
| Male | Mean | 48.99 | 49.03 | 54.96 | 56.25 | 42.11 | 56.40 |
| SD | 26.06 | 23.29 | 34.80 | 34.53 | 26.27 | 22.37 | |
| Female | Mean | 48.87 | 48.84 | 55.78 | 56.12 | 42.65 | 56.14 |
| SD | 26.02 | 23.28 | 35.09 | 35.29 | 26.18 | 22.42 | |
| p-value | >0.05 | >0.05 | >0.05 | >0.05 | >0.05 | >0.05 | |
| SOFA scores | |||||||
| <8 | Mean | 48.95 | 49.33 | 54.52 | 55.71 | 42.09 | 56.43 |
| SD | 26.95 | 23.38 | 34.97 | 34.80 | 26.15 | 22.37 | |
| ≥ 8 | Mean | 48.90 | 49.33 | 54.36 | 55.66 | 42.47 | 56.4 |
| SD | 26.17 | 23.38 | 35.11 | 34.80 | 26.12 | 22.38 | |
| p– value | >0.05 | >0.05 | <0.05* | >0.05 | >0.05 | >0.05 |
*Statistical significance
Table 13 shows that our study correlated various domains of SF 20 questionnaire with different variable such as age, gender and SOFA scores. The mean±SD was calculated for each domain. All the age group showed poor health perception with mean below 50 except patients aged between 25 – 34 y, whereas all the other age groups showed decreased social functioning. Both the genders revealed poor health perception and decreased social functioning as well the patients with SOFA score with<8 and ≥ 8. The association of different age groups with SF 20 domains was carried out using ANOVA statistics. The two domains, physical functioning and Role functioning showed statistical significance i. e., the physical functioning and role functioning varied among different age groups with p-value<0.01 and<0.05, respectively, whereas other domains did not show statistical significance.
The relation between domains of SF 20 among two genders and SOFA score<8 and ≥ 8 was performed using T statistics. The test showed no statistical significance in any of the domains among the two genders whilst physical functioning revealed statistical significance among SOFA scores<8 and ≥ 8.
DISCUSSION
In this prospective observational study, the prevalence of sepsis was higher among male patients over females, which was corresponding to a study done by Jain P et al., [11], where the prevalence of sepsis in males and females was 63.8% and 36.2%, respectively. Another prospective study by Saha DK et al., [22] observed 52.2% and 47.8% of males and females sepsis patients respectively, similar to data obtained from studies conducted by Dewi RS et al., [23] and Gopala K et al., [13]. The underlying cause of the male predominance in sepsis prevalence remains elusive and warrants further investigation. The majority of the patients belonged to the age group of 55 – 64 y. The mean age was found to be 54.09±16.14 y (mean±SD), which indicated that elderly people are more vulnerable to developing sepsis. Saha DK et al., [22] observed that the mean age was 58.25±15.03 y’ studies showing predominance of sepsis in age group 61-70 y. Our study examined relation between various age groups and sources of infection and the relation between age and length of stay (LOS), which showed no statistical significance between the respective variables.
In this study, the prescribing patterns of empirical therapy for sepsis patients were meticulously analyzed, with a focus on categorizing antibiotics according to the WHO AWaRe Classification within a tertiary care hospital setting. The analysis not only delved into the antibiotic categories but also scrutinized their placement within the Access, Watch, and Reserve Classes. It was observed that the Watch class antibiotics were administered at the highest rate, followed by the Access class, and then the Reserve class. A multi-centre, cross-sectional study conducted by Dat VQ et al., [9] in Vietnam noted that a substantial proportion of CCU patients received antibiotics from the Watch category, while Access and Reserve antibiotics were prescribed to a lesser extent. Moreover, our study highlighted the use of monotherapy over combination therapy, wherein 107 antibiotics were administered empirically, predominantly falling within the Watch category. Combination therapy, involving two drugs, exhibited a higher frequency within the Watch category, followed by combinations of Access and Watch, and Watch and Reserve. Similarly, a Point Prevalence survey conducted in Bangladesh by Rashid MM et al., [10] with 1417 participants showcased a preference for monotherapy involving antibiotics, followed by combination therapy involving two or three antibiotics. These findings collectively emphasize the diverse prescribing practices and trends in antibiotic usage across different healthcare settings and geographic regions.
Our study exhibited prevalence of g-negative organisms, which was similar to study done by Jain P et al., [11]. The resistant pathogens were identified to be fairly common wherein, K. pneumoniae of g-negative category, was highly resistant to multiple empirical drugs of choice, except for Linezolid highlighting the adaptability of bacteria in developing resistance mechanisms. A cohort study undertaken by Rhee C et al. [2] assessed the prevalence of antibiotic-resistant pathogens in patients with culturally proven, community-onset sepsis receiving broad spectrum empiric antibiotics. However resistant pathogens were relatively uncommon-where the net prevalence of at least 1 resistant g-positive organism was 13.6%, so the overall prevalence of antibiotic resistance was comparatively low. The most common source of infection in this study was respiratory infection, followed by those of which the source remained unidentified, skin and urinary-tract infections. A total of 18 antibiotics were employed to counter various infections, of which the most frequently used were Piperacillin/Tazobactam and Meropenem. On the basis of results of the microbial cultures and antibiotic susceptibility tests, Ceftriaxone, Cefoperazone/Sulbactam and Meropenem presented with higher resistance rates, examining its contributions as empirical therapy and thereby, the pattern of antibiotic use in disease management involving antibiotics with high resistance.
The influence of age in relation to bacteria growth revealed significant association. A highly significant association derived between bacterial growth and AWaRe categories of empirical therapy using Chi Square test, underscores the importance of selecting the right antibiotics early on and the need for continuous monitoring of resistance patterns to improve patient outcomes. In a similar retrospective, observational study conducted by Pradipta IS et al. [12] involving 192 participants, identified lungs as the primary source of sepsis infection. 47 antibiotics were utilized in the study of which 61.35% of the antibiotics used showed resistance rates more than 50%. The selection of an inappropriate empirical antibiotic therapy conformed to mortality rate, longer duration of hospitalization and a high incidence of multidrug resistance (MDR).
The association between SOFA scores with LOS and clinical outcome was carried out in our research. The result of study showed admission SOFA score and Length of stay followed by survival and non survival. In our study the association between mean LOS with survival and non survival did not show statistical significance similar to Tekade et al., [15]. Conversely the association between mean admission SOFA score with survival and non survival showed no statistical significance whereas the Takeda et al., [15] study observed higher significance. The current study, observed that the correlation between admission SOFA scores and LOS was statistically significant as observed in the study conducted by Takeda et al., [15] and also the study done by Karnina R et al., [16] showed association between two variables. The correlation of SOFA score with clinical outcome revealed not statistically significant. The SOFA score changes over the time and needs further studies to be done including the change over SOFA scores. The Association of SOFA scores with age and gender respectively showed no statistical significance.
On evaluating the health-related quality-of-life in sepsis survivors using SF-20 questionnaire by correlating all Age groups, physical and role functioning results showed statistical significance among various age groups. Gender had no significant influence on any domains of SF 20, similar to a cross-sectional study conducted by Baghianimoghadam MH et al., [19]. Patients with both<8 and ≥ 8 SOFA Scores reported of poor health perception and decreased social functioning, suggesting that the severity of organ dysfunction or failure did not significantly alter these perceptions among the participants and that it continues to be consistent among all levels of organ dysfunction severity.
CONCLUSION
This study investigated 174 ICU sepsis patients, revealing major concerns of irrational over reliance of broad-spectrum empirical antibiotics, posing a significant risk of fostering antibiotic resistance which essentially deviates from the WHO "Access class" guidelines. The pattern of microbial culture in association with antimicrobial resistance revealed, g negative bacteria as the leading source of infection with high resistance levels to the most commonly used antibiotics, highlighting the urgent need for an enhanced antimicrobial stewardship in sepsis management. While higher SOFA scores were associated with prolonged hospitalization, indicating their potential as an indicator of disease severity, the correlation between SOFA scores and clinical outcomes were weak, highlighting the complexity of sepsis and the multi-factorial nature of patient outcomes emphasising the need for a comprehensive approach that extends beyond initial physiological scores. Furthermore, Health-Related Quality of Life (HRQoL) assessments via the SF-20 questionnaire, demonstrated that sepsis inflicts profound, long-term damage on physical, social, and mental capabilities, signaling that the duty of care must extend beyond hospitalisation to improve patient survival status. Ultimately this study highlights that improving sepsis outcomes requires a holistic shift towards judicious antibiotic stewardship and the need for robust post discharge support to address the long term impacts of sepsis.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCES
World Health Organization. Global report on the epidemiology and burden of sepsis: current evidence identifying gaps and future directions. Geneva: World Health Organization; 2020. Available from: https://www.who.int/publications/i/item/9789240010789. [Last accessed on 12 Jan 2024].
Rhee C, Kadri SS, Dekker JP, Danner RL, Chen HC, Fram D. Prevalence of antibiotic-resistant pathogens in culture-proven sepsis and outcomes associated with inadequate and broad-spectrum empiric antibiotic use. JAMA Netw Open. 2020;3(4):e202899. doi: 10.1001/jamanetworkopen.2020.2899, PMID 32297949.
Pauwels I, Versporten A, Drapier N, Vlieghe E, Goossens H, Global-PPS Network. Hospital antibiotic prescribing patterns in adult patients according to the WHO access, watch and reserve classification (AWaRe): results from a worldwide point prevalence survey in 69 countries. J Antimicrob Chemother. 2021 May 12;76(6):1614-24. doi: 10.1093/jac/dkab050, PMID 33822971.
World Health Organization. AWaRe classification of antibiotics for evaluation and monitoring of use. Geneva: World Health Organization; 2023. Available from: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.04. [Last accessed on 13 Jan 2024].
Van Der Slikke EC, Beumeler LF, Holmqvist M, Linder A, Mankowski RT, Bouma HR. Understanding post-sepsis syndrome: how can clinicians help? Infect Drug Resist. 2023 Sep 29;16:6493-511. doi: 10.2147/IDR.S390947, PMID 37795206.
Al-Sunaidar KA, Prof Abd Aziz N, Prof Hassan Y. Appropriateness of empirical antibiotics: risk factors of adult patients with sepsis in the ICU. Int J Clin Pharm. 2020 Apr;42(2):527-38. doi: 10.1007/s11096-020-01005-4, PMID 32144611.
Garg R, Tellapragada C, Shaw T, Eshwara VK, Shanbhag V, Rao S. Epidemiology of sepsis and risk factors for mortality in intensive care unit: a hospital based prospective study in South India. Infect Dis (Lond). 2022;54(5):325-34. doi: 10.1080/23744235.2021.2017475, PMID 34986756.
Hammond NE, Kumar A, Kaur P, Tirupakuzhi Vijayaraghavan BK, Ghosh A, Grattan S. Estimates of sepsis prevalence and outcomes in adult patients in the ICU in India: a cross-sectional study. Chest. 2022 Jun;161(6):1543-54. doi: 10.1016/j.chest.2021.12.673, PMID 35092747.
Dat VQ, Dat TT, Hieu VQ, Giang KB, Otsu S. Antibiotic use for empirical therapy in the critical care units in primary and secondary hospitals in Vietnam: a multicenter cross-sectional study. Lancet Reg Health West Pac. 2021 Nov 3;18:100306. doi: 10.1016/j.lanwpc.2021.100306, PMID 35024650.
Rashid MM, Akhtar Z, Chowdhury S, Islam MA, Parveen S, Ghosh PK. Pattern of antibiotic use among hospitalized patients according to WHO access watch reserve (AWaRe) classification: findings from a point prevalence survey in Bangladesh. Antibiotics (Basel). 2022;11(6):810. doi: 10.3390/antibiotics11060810, PMID 35740216.
Jain P, Galiya A, Luke Philip S, Mateti UV, P SS, Gudi SK. Bacteriological profile and antimicrobial resistance pattern among patients with sepsis: a retrospective cohort study. Int J Clin Pract. 2021;75(10):e14701. doi: 10.1111/ijcp.14701, PMID 34351692.
Pradipta IS, Sodik DC, Lestari K, Parwati I, Halimah E, Diantini A. Antibiotic resistance in sepsis patients: evaluation and recommendation of antibiotic use. N Am J Med Sci. 2013 Jun;5(6):344-52. doi: 10.4103/1947-2714.114165, PMID 23923107.
Gopala K, Kumar S, Ravi S, Kondle R, Vemula S, Pasupuleti S. Sequential organ failure assessment and modified early warning score system versus quick SOFA score to predict the length of hospital stay in sepsis patients-accuracy scoring study. Crit Care Innov. 2021;4(4):9-18. doi: 10.32114/CCI.2021.4.4.9.18.
Li Y, Yan C, Gan Z, Xi X, Tan Z, Li J. Prognostic values of SOFA score, qSOFA score, and LODS score for patients with sepsis. Ann Palliat Med. 2020 May;9(3):1037-44. doi: 10.21037/apm-20-984, PMID 32498525.
Tekade T, Manohar T. Utility of SOFA (sequential organ function assessment) score to predict outcome in critically ill patients at a Tertiary Care Hospital, Nagpur. Panacea J Med Sci. 2017;7(3):140-6. doi: 10.18231/2348-7682.2017.0037.
Karnina R, Sugiarto A, Manggala SK, Yulasutu B. Relationship between SOFA score and length of hospitalization for sepsis patients in the intensive care unit of a single institution. Bali Med J. 2024;13(1):653-6556. doi: 10.15562/bmj.v13i1.4913.
Mishra R, Chakrabarty J, Sequria L. A study to assess the patient clinical outcome using sofa score among patients admitted to ICU of tertiary hospital of South India. Int J Health Sci Res. 2018;8(2):164-70. doi: 10.52403/ijhsr.
Jain A, Palta S, Saroa R, Palta A, Sama S, Gombar S. Sequential organ failure assessment scoring and prediction of patient’s outcome in intensive care unit of a tertiary care hospital. J Anaesthesiol Clin Pharmacol. 2016 Jul-Sep;32(3):364-8. doi: 10.4103/0970-9185.168165, PMID 27625487.
Baghianimoghadam MH, Afkhami AM, Ardekani M, Baghianimoghadam B. Effect of education on improvement of quality of life by SF-20 in type 2 diabetic patients. Acta Med Indones. 2009 Oct;41(4):175-80. PMID 20124612.
Stein MD, Mulvey KP, Plough A, Samet JH. The functioning and well being of persons who seek treatment for drug and alcohol use. J Subst Abuse. 1998;10(1):75-84. doi: 10.1016/S0899-3289(99)80142-4, PMID 9720008.
Baghianimoghadam MH, Sharifirad G, Rahaei Z, Baghianimoghadam B, Heshmati H. Health related quality of life in children with thalassaemia assessed on the basis of SF-20 questionnaire in Yazd, Iran: a case-control study. Cent Eur J Public Health. 2011 Sep;19(3):165-9. doi: 10.21101/cejph.a3640, PMID 22026294.
Saha DK, Saha M, Ahsan AA, Fatema K, Ahmed F, Nazneen S. Prognostic value of SOFA score and SIRS criteria for ICU mortality in adult sepsis patients admitted to the ICU of a Tertiary Care Hospital of Bangladesh. BIRDEM Med J. 2021;11(2):84-9. doi: 10.3329/birdem.v11i2.53130.
Dewi RS, Radji M, Andalusia R. Evaluation of antibiotic use among sepsis patients in an intensive care unit: a cross-sectional study at a referral hospital in Indonesia. Sultan Qaboos Univ Med J. 2018;18(3):e367-73. doi: 10.18295/squmj.2018.18.03.017, PMID 30607280.