
Int J Curr Pharm Res, Vol 18, Issue 1, 10-13Original Article
APPROPRIATENESS OF FRESH FROZEN PLASMA TRANSFUSION-A RETROSPECTIVE ANALYSIS
MANIMOZHI M.1, PARIMALAM M.2, RAVISHANKAR J.3*
1Department of Immunohematology and Blood Transfusion, Government Ramanathapuram Medical College, Ramanathapuram, Tamilnadu, India. 2,3*Department of Immunohematology and Blood Transfusion, Tirunelveli Medical College, Tirunelveli, Tamilnadu, India
*Corresponding author: Ravishankar J.; *Email: ravishankar@tvmc.ac.in
Received: 06 Oct 2025, Revised and Accepted: 26 Nov 2025
ABSTRACT
Objective: Every blood component carries inherent risk of adverse transfusion reactions and transfusion-transmitted infections (TTI). As Fresh frozen plasma (FFP) is one of the commonly used blood components, appropriate and rational use is necessary for patient safety. The objective of the study was to evaluate the appropriateness of FFP utilization in clinical practice.
Methods: This retrospective study was conducted at the Department of Immunohematology and Blood Transfusion, Tirunelveli Medical College and Hospital, Tirunelveli, Tamilnadu, India in June, 2024. Blood Request Forms with request for FFP transfusion between December 2023 and May 2024 were analysed. Data entry and statistical analysis was performed using Microsoft Excel sheet.
Results: 631 patients received 1798 FFP units (mean=2.85 units), 16.1% of transfusions were in the age group of 31-40 years (n=291/1798), 53.6% were in males (n=963/1798), 27.5% were issued to the Department of General medicine (n=495/1798). 65.1% of transfusions were appropriate (n=1171/1798), the most common indication being therapeutic plasma exchange. Inappropriate transfusion indications were for volume replacement, to improve wound healing and prophylactic use during surgeries.
Conclusion: As FFP is involved more in adverse transfusion reactions like allergy and Transfusion-related acute lung injury (TRALI), inappropriate indications can be reduced significantly with continuous education of end users by regular CMEs, interactive sessions, discussion in Hospital transfusion committee and prospective audits, to ensure optimal use of the scarce resource and to reduce transfusion-related adverse events.
Keywords: Appropriateness, Fresh frozen plasma, Transfusion reaction
© 2026 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2026v18i1.7088 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Fresh frozen plasma (FFP) is a commonly transfused blood component that contains plasma proteins and full spectrum of coagulations factors, including the labile factors V and VIII. Transfusion of FFP is primarily recommended in clinical situations associated with coagulation abnormalities [1]. Every blood component carries inherent risk of adverse transfusion reactions including TTI [2]. Inappropriate request from clinicians and unnecessary use of FFP increases the risk of side effects like excess volume replacement, anaphylaxis, microbes transmitted through transfusion and TRALI in patients [3]. There is a shortage of blood components in most of the developing countries. But the demand for blood components is ever-increasing. Appropriate use of blood and blood components is necessary to ensure their availability for needy patients as well as to avoid the unnecessary risk of transfusion-transmitted diseases [4, 5].
Each donation of whole blood can be separated to as many as four different components (packed red cell concentrate, platelet concentrate, fresh frozen plasma and cryoprecipitate) that can be transfused to patients. FFP is the plasma unit isolated from one unit of whole blood (450 ml) and rapidly frozen within eight hours from donation. FFP usually measures 200-220 ml and it contains 70–80 units of factor VIII, IX, Von Will brand Factor (VWF) and other clotting factors [6]. Infusion of 10-15 ml/kg body weight of the patient is considered an adequate dose [7].
FFP is indicated in conditions such as coagulation deficiency secondary to liver disease, disseminated intravascular coagulation, dilutional coagulopathy due to massive blood transfusion, in pediatric population with primary or secondary immunodeficiency, anti-thrombin deficiency and open-heart surgery [6]. FFP contains antibodies and is capable of causing complications like haemolytic transfusion reactions (due to ABO antibodies) and TRALI and also capable of transmitting pathogens. Allergic reactions and fluid overload are also common with plasma infusion. Hence, FFP transfusion is not without complications [8, 9].
Despite the advancements in quality control, standardization and available guidelines about use of FFP, there are many studies which report a higher occurrence of inappropriateness while ordering this blood component [8]. The British Society for Hematology have published guidelines to highlight these issues and minimize the misuse [10]. Literature search revealed only a few audits from India. These guidelines also recommend that response to transfusion of blood components should be monitored by clinical evaluation and lab parameters to make further treatment decisions. It is also recommended that the recipient of blood component should be closely monitored for any adverse transfusion reaction [11]. The published reports on FFP utilization have focused predominantly on the appropriateness of FFP transfusions to improve the patient outcome [1, 12, 13]. Very few studies have thrown light on the monitoring of transfusion events [4, 14].
MATERIALS AND METHODS
This was a retrospective cross-sectional study conducted at a single centre, Department of Immunohematology and Blood Transfusion, Tirunelveli Medical College and Hospital, Tirunelveli, Tamilnadu, India in June 2024. Blood Request Forms with request for FFP transfusion between December 2023 and May 2024 were analysed, after obtaining Institutional Ethics Committee approval. All data were collected from blood request forms; crossmatch register and issue register at Blood centre. Information collected included demographic data, including age and gender, clinical diagnosis, departments requesting FFP, number of units transfused and patient’s coagulation profile, if any. FFP transfusion guidelines as per British Committee for standards in Hematology 2004 and 2018 (review), was followed to differentiate appropriate from inappropriate FFP transfusion indications [10]. Data entry and statistical analysis was performed using Microsoft Excel sheet.
RESULTS
A total of 1798 units of FFP were issued to 631 patients during study period. Most of the patients belonged to 31-40 age group (24.88%, n = 157/631) (fig. 1). Mean age of the patient population was 36.88±16.5 years. Males were nearly equal to females (52.77%, n = 333/631). Mean number of units transfused per patient was 2.85±1.47.
FFP was most commonly transfused in the age group of 31-40 years (24.2%, n = 436/1798). 53.5% of FFP transfusions were received by male patients (n = 963/1798 units) (fig. 2). More FFP transfusions were performed at Department of General Medicine (n=495/1798, 27.5%) and Department of Pediatrics (n=476/1798, 26.6%) (fig. 3). 65.1% (n=1171/1798) of total FFP utilization were appropriate transfusions and most were done at the Department of General medicine (73.9%). Most of the inappropriate transfusions were done at the department of Orthopedics (48.2%) (table 1). Most common indication for appropriate transfusion was therapeutic plasma exchange. Indications for Inappropriate transfusion were volume replacement and to improve wound healing (table 2).
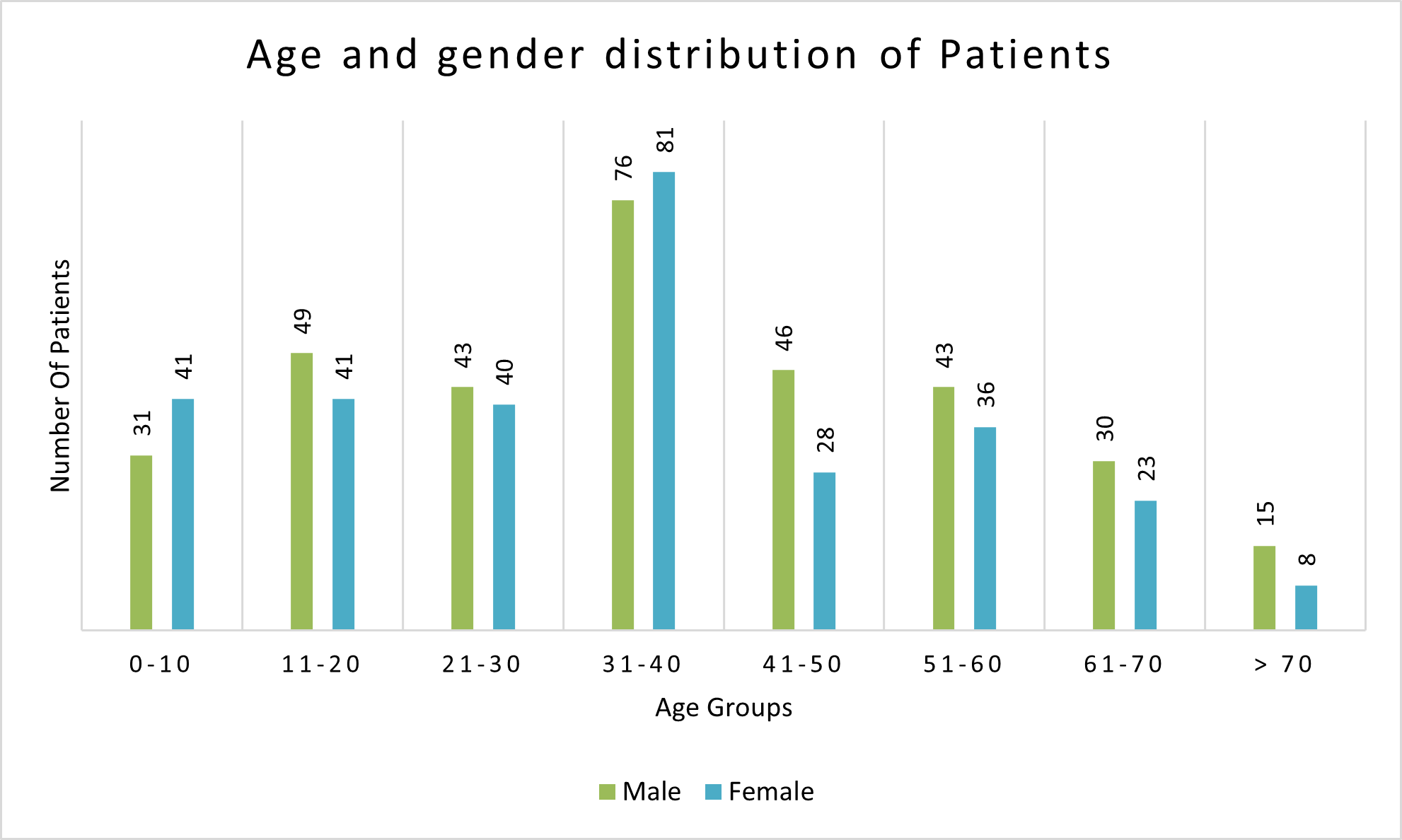
Fig. 1: Age and gender distribution of patients who had received FFP transfusion (age group in years and gender in numbers)
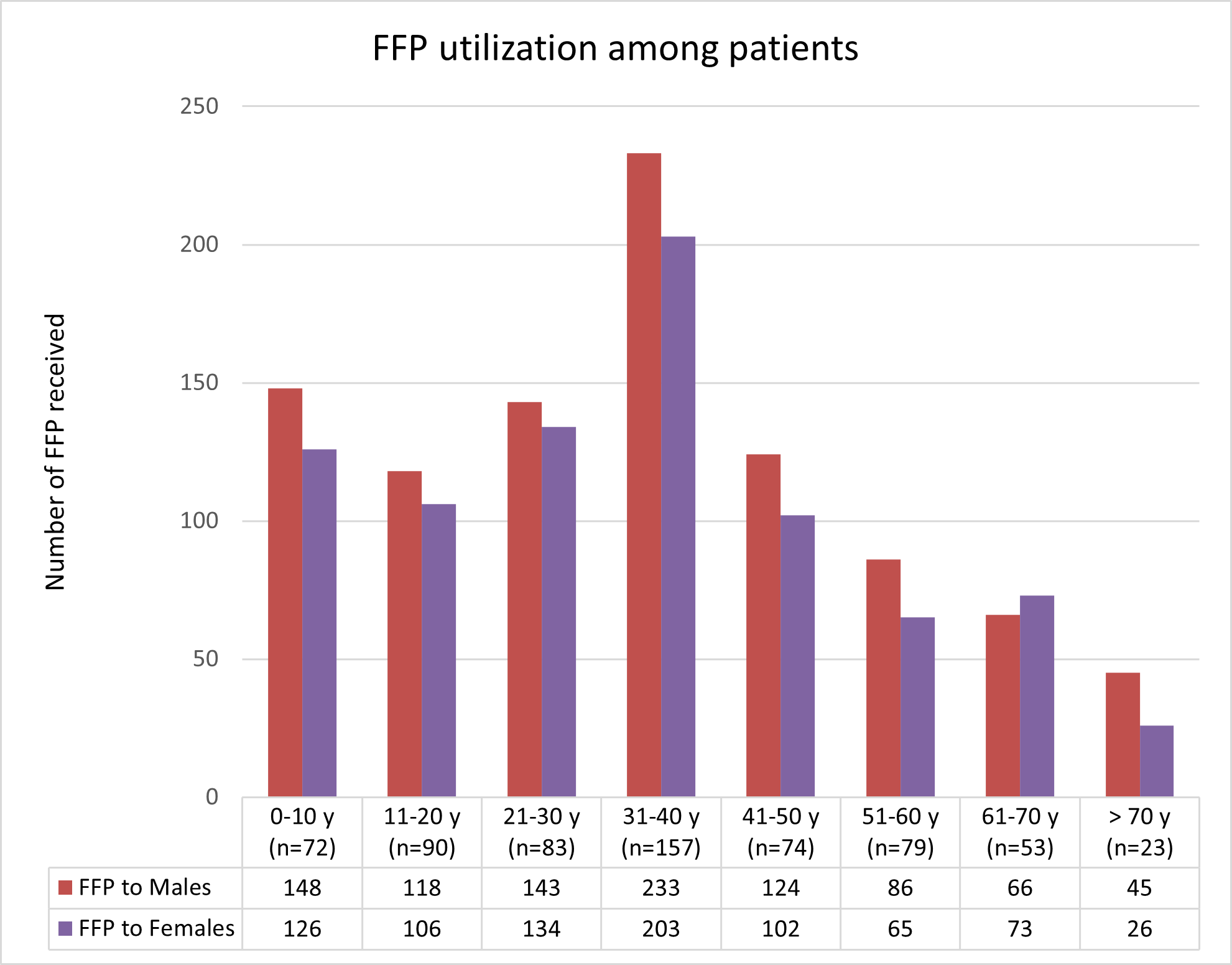
Fig. 2: Number of FFP transfused in patients across age groups and gender [age group in years and number of patients in each age group (n) is given in brackets]
Table 1: Specialty-wise categorization of transfusion appropriateness
| S. No. | Department | Total FFP units issued | Appropriate transfusions (n, %) | Inappropriate transfusions (n, %) |
| 1 | General Medicine | 495 | 366(73.9%) | 129(26.1%) |
| 2 | Pediatrics | 476 | 302(63.4%) | 174(36.5%) |
| 3 | General Surgery | 276 | 165(59.7%) | 111(40.2%) |
| 4 | Obsand Gynae | 245 | 141(57.5%) | 104(42.4%) |
| 5 | TAEI | 102 | 72(70.5%) | 30(29.4%) |
| 6 | Orthopedics | 58 | 30(51.7%) | 28(48.2%) |
| 7 | Others (including burns) | 146 | 95(65.1%) | 51(34.9%) |
(Number of transfusions are given in numbers (n) and percentage of total FFP transfusions), (TAEI – Tamilnadu Accident and Emergency care Initiative)
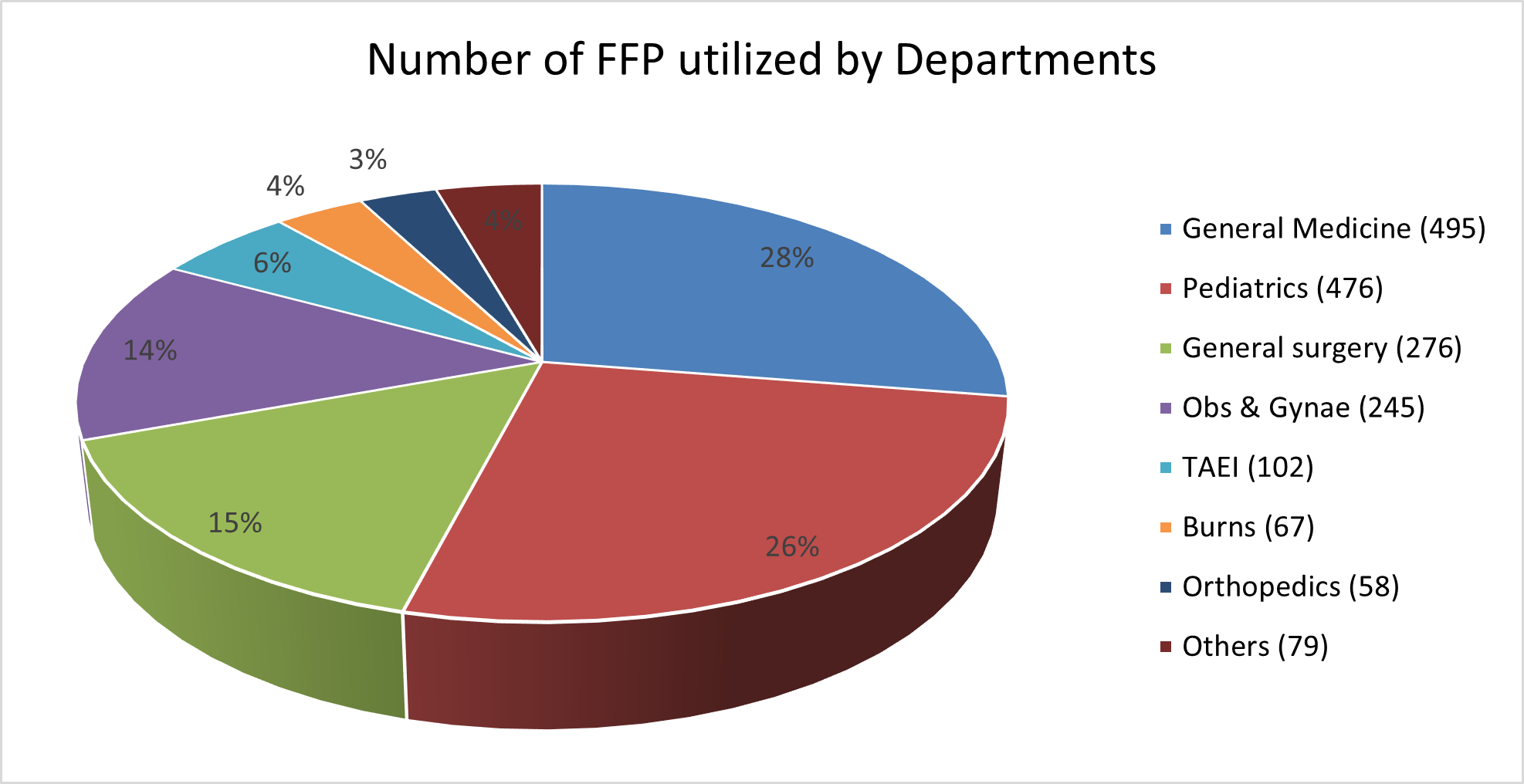
Fig. 3: Specialty-wise utilization of FFP (given as percentage of total FFP utilized)
Table 2: Indications for appropriate and inappropriate FFP transfusions seen in major user specialty departments
| Individual department | Common indications of appropriate FFP transfusion | Common indications of inappropriate FFP transfusion |
| General medicine | Therapeutic Plasma exchange, warfarin reversal, elevated INR, liver disease with altered coagulopathy. | Fever with thrombocytopenia, hypoproteinemia, sepsis |
| General surgery | Major surgeries with bleeding. | Volume replacement, wound healing |
| Pediatrics | Major surgeries, sepsis and conditions with bleeding risk. | Intra Ventricular Hemorrhage, thrombocytopenia, Shock. |
| Obs and gynae | Antepartum and postpartum hemorrhage | Volume replacement, jaundice without coagulopathy. |
DISCUSSION
Fresh frozen plasma is a frequently transfused blood component and evaluation of FFP usage is considered an important and valid method for improving the appropriate utilization of FFP. Contrary to belief among many clinicians, FFP transfusions are not risk-free. Allergic reactions, TRALI and TTIs can all be caused by FFP transfusions. They were also reported when convalescent plasma therapy was tried in Covid-19 patients [15].
According to British Committee for Standards in Haematology guidelines, [16] bleeding history, including family history, details of prior surgeries and anticoagulant treatment should be taken prior to surgery. Patients with a negative bleeding history do not require routine preoperative coagulation testing. The threshold of Prothrombin time (PT) and activated plasma thromboplastin time (aPTT) prolongation of>1-1.5 times normal was based on outdated retrospective studies, and PT and aPTT themselves are poor predictors of perioperative bleeding, especially in patients with a negative bleeding history [4, 14, 17]. However, some recent papers still recommend routinely performing PT, aPTT and platelet count prior to surgery and invasive procedures in adults and children. FFP transfusion is considered appropriate in patients with excessive warfarin effect only if they have a massive bleeding or have emergency surgery [4, 11]. Prothrombin complex concentrate (PCC) is effective in reversing the effect of warfarin and FFP may be used when there is severe bleeding and PCC is not available.
In the present study, FFP was most commonly transfused in the age group of 31-40 years (24.2%). In a similar retrospective study by Shinagare et al., FFP was most often used in patients of age range 16–30 years [4]. In the present study, more FFP transfusions were done in the department of general medicine (27.5%) while in the study by Agarwal et al., Neurosurgery Department utilized more FFP units (46.9 %) [18]. But in the study by Shinagare et al. Department of Obstetrics and Gynaecology utilized most units of FFP [4].
In spite of clear guidelines, many studies have shown a higher incidence of inappropriate use of FFP. In the present study, 65.1% (n= 1171/1798) were appropriate transfusions. The common appropriate indications were use of FFP in therapeutic plasma exchange, liver disease with altered coagulopathy, surgical bleeding and obstetric hemorrhage. While the study by Pratibha et al. demonstrated appropriate use of FFP in 40%, the study by Iorio et al. showed that the indication was appropriate in only 31.5 % of the requests [19, 7]. A recent prospective analysis by Akkas¸ M et al., reported inappropriate use of FFP in 67 % of transfusions [20]. In the present study, most of the inappropriate indications was seen at the Department of Orthopedics (48.2%). This was similar to study done by Agarwal et al., where the inappropriate usage was seen morein orthopedic patients (69.3 %) [18]. In the study by Makroo et al., the most common indications were surgical bleeding, liver disease and massive transfusion [21]. This inappropriateness is compounded by inadequate reporting of transfusion reactions [22].
In this study, 34.9 % of FFP transfusions were inappropriate in various departments along with inadequacy of transfusion documentation. One of the indications was to treat hypoproteinemia when 5% albumin was unavailable. This can be addressed by ensuring adequate supply of 5% albumin in Government hospitals.
CONCLUSION
To ensure the optimal use of the scarce resource and to reduce transfusion-related adverse events, regular transfusion audits and continuous education of end users by regular CMEs are to be conducted. Awareness has to be created and encouraging blood ordering departments to participate in patient blood management program can be recommended. Regular Hospital Transfusion committee meetings with discussion of guidelines and continuous monitoring of clinical departments for adherence will improve appropriate utilization of blood and blood components. Blood request forms can be updated to carry indications for blood components or transfusion thresholds, to remind physicians about appropriate usage of FFP.
ACKNOWLEDGMENT
The authors would like to acknowledge all staff at the blood centre for their cooperation and support in conducting this study.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
MM conceptualized the study, collected data and prepared manuscript. PM edited manuscript and analyzed data. JR analyzed data and accepted manuscript.
CONFLICT OF INTERESTS
Declared none
REFERENCES
Bhagwat SN, Sharma JH. A retrospective audit of appropriateness and monitoring of fresh frozen plasma transfusions in a Tertiary Care Hospital. Int J Contemp Med Res. 2017;4(7):1562-7.
Yadav A, Tiwari P, Sheemar AK. An audit on usage of fresh frozen plasma in a Tertiary Care Hospital in North Western part of India. Int J Res Med Sci. 2020;9(1):106-11. doi: 10.18203/2320-6012.ijrms20205663.
Kleinman S, Caulfield T, Chan P, Davenport R, McFarland J, McPhedran S. Toward an understanding of transfusion-related acute lung injury: statement of a consensus panel. Transfusion. 2004;44(12):1774-89. doi: 10.1111/j.0041-1132.2004.04347.x, PMID 15584994.
Shinagare SA, Angarkar NN, Desai SR, Naniwadekar MR. An audit of fresh frozen plasma usage and effect of fresh frozen plasma on the pre-transfusion international normalized ratio. Asian J Transfus Sci. 2010;4(2):128-32. doi: 10.4103/0973-6247.67024, PMID 20859514.
World Health Organization. Blood safety and availability. Geneva: World Health Organization; 2023 Jun 2. Available from: https://www.who.int/news-room/fact-sheets/detail/blood-safety-and-availability. [Last accessed on 22 Dec 2025].
Gurevitz SA. Update and utilization of component therapy in blood transfusions. Lab Med. 2010;41(12):739-44. doi: 10.1309/lmhv0yr52ibvijaa.
Iorio A, Basileo M, Marchesini E, Materazzi M, Marchesi M, Esposito A. The good use of plasma. A critical analysis of five international guidelines. Blood Transfus. 2008;6(1):18-24. doi: 10.2450/2008.0041-07, PMID 18661920.
Jayanthi N, Pitchai R. Audit of fresh frozen plasma usage and study the effect of fresh frozen plasma on the pre-transfusion and post-transfusion international normalized ratio. Int J Curr Med Appl Sci. 2015;7(1):34-9.
Bjerrum OJ, Jersild C. Class-specific anti-IgA associated with severe anaphylactic transfusion reactions in a patient with pernicious anaemia. Vox Sang. 1971;21(5):411-24. doi: 10.1111/j.1423‑0410.1971.tb04797.x.
Green L, Bolton Maggs P, Beattie C, Cardigan R, Kallis Y, Stanworth SJ, Zahra S. British Society of Haematology guidelines on the spectrum of fresh frozen plasma and cryoprecipitate products: their handling and use in various patient groups in the absence of major bleeding. Br J Haematol. 2018;181(1):54-67. doi: 10.1111/bjh.15167, PMID 29527654.
O’Shaughnessy DF, Atterbury C, Bolton Maggs P, Murphy M, Thomas D, Yates S. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126(1):11-28. doi: 10.1111/j.1365-2141.2004.04972.x, PMID 15198728.
Ravishankar J, Jagannathan SY, Arumugam P, Chitra M. Evaluating the appropriateness of blood component utilization in burns patients. Int J Res Med Sci. 2016 Dec 16;4(12):5364-71. doi: 10.18203/2320‑6012.ijrms20164211.
Hui CH, Williams I, Davis K. Clinical audit of the use of fresh-frozen plasma and platelets in a Tertiary Teaching Hospital and the impact of a new transfusion request form. Intern Med J. 2005;35(5):283-8. doi: 10.1111/j.1445-5994.2005.00803.x, PMID 15845110.
Holland LL, Brooks JP. Toward rational fresh frozen plasma transfusion: the effect of plasma transfusion on coagulation test results. Am J Clin Pathol. 2006;126(1):133-9. doi: 10.1309/NQXH-UG7H-ND78-LFFK, PMID 16753596.
Taurustya H, Yunita S, Ysrafil Y, Pratiwi N, Rahmatiah A. Lessons and new perspectives: is convalescent plasma therapy effective on COVID-19 patients? Int J App Pharm. 2022 Jan 7;14(1):50-7. doi: 10.22159/ijap.2022v14i1.42452.
Chee YL, Crawford JC, Watson HG, Greaves M. Guidelines on the assessment of bleeding risk prior to surgery or invasive procedures. Br J Haematol. 2008;140(5):496-504. doi: 10.1111/j.1365-2141.2007.06968.x, PMID 18275427.
Ewe K. Bleeding after liver biopsy does not correlate with indices of peripheral coagulation. Dig Dis Sci. 1981;26(5):388-93. doi: 10.1007/BF01313579, PMID 7249879.
Agarwal N, Subramanian A, Pandey RM, Albert V, Karjee S, Arya V. An audit of fresh frozen plasma usage in a tertiary trauma care centre in north India. Indian J Hematol Blood Transfus. 2014;30(4):328-32. doi: 10.1007/s12288-013-0265-0, PMID 25435737.
Prathiba R, Jayaranee S, Ramesh JC, Lopez CG, Vasanthi N. An audit of fresh frozen plasma usage in a tertiary referral centre in a developing country. Malays J Pathol. 2001;23(1):41-6. PMID 16329547.
Akkas M, Ataman D, Akman C, Aksu NM, Karaca MA, Aksu S. Inappropriate fresh frozen plasma use in coagulation disorder. Eur J Surg Sci. 2011;2(2):38-41.
Makroo RN, Raina V, Kumar P, Thakur UK. A prospective audit of transfusion requests in a Tertiary Care Hospital for the use of fresh frozen plasma. Asian J Transfus Sci. 2007 July;1(2):59-61. doi: 10.4103/0973-6247.33847, PMID 21938235.
Swetha K, Vishnu. Knowledge, attitude and application of hemovigilance by postgraduates and interns in a Tertiary Care Hospital. Int J Pharm Pharm Sci. 2024 July;16(7):36-9. doi: 10.22159/ijpps.2024v16i7.51206.