
Int J Curr Pharm Res, Vol 18, Issue 1, 76-79Original Article
QUANTITATIVE ASSESSMENT OF SKIN STIFFNESS AND THICKNESS USING HIGH-FREQUENCY ULTRASOUND AND SHEAR WAVE ELASTOGRAPHY IN THE MANAGEMENT OF SCLERODERMA: A PROSPECTIVE COMPARATIVE STUDY
SUDHA MADHURI BASABOINA1*, NIKHIL DESHNENI2
1Department of Dermatology Venereology and Leprosy, Dr. Patnam Mahender Reddy Institute of Medical Sciences, Hyderabad, Telangana. 2Department of Radiodiagnosis, Dr. Patnam Mahender Reddy Institute of Medical Sciences, Hyderabad, Telangana
*Corresponding author: Sudha Madhuri Basaboina; *Email: drsudhamadhuri11@gmail.com
Received: 10 Oct 2025, Revised and Accepted: 28 Nov 2025
ABSTRACT
Objective: The objective of this study is to analyze skin stiffness and thickness quantitatively in patients with systemic sclerosis using high-frequency ultrasound (HFUS) and shear wave elastography (SWE), and to compare those results with healthy controls. This study aims to examine the diagnostic utility, examine the performance between both modalities and determine their correlation with modified Rodnan skin score (mRSS), and establish their clinical utility in the early diagnosis and monitoring of disease severity in scleroderma.
Methods: In this observational study, skin stiffness and thickness were assessed in SSc patients and matched healthy controls using HFUS and SWE. Quantitative measurements were taken at standard anatomical sites. Receiver operating characteristic (ROC) curve analysis evaluated the diagnostic accuracy of each modality, while correlation with the modified Rodnan skin score (mRSS) was analyzed to determine clinical relevance.
Results: Both skin thickness and stiffness were significantly elevated in SSc patients compared to controls (p<0.001). SWE exhibited superior diagnostic accuracy (AUC 0.881) compared to HFUS (AUC 0.795), with sensitivities of 90% and 82%, respectively. Strong positive correlations were observed between imaging parameters and mRSS (r = 0.758 for SWE stiffness; r = 0.642 for HFUS thickness).
Conclusion: HFUS and SWE constitute effective, complementary tools for quantitative evaluation of skin involvement in systemic sclerosis. Their combined use improves diagnostic precision and correlates well with clinical skin scores, supporting integration into routine clinical assessment and trials. Further multicenter validation and protocol standardization are warranted.
Keywords: Systemic sclerosis, High-frequency ultrasound, Shear wave elastography, Skin stiffness, Skin thickness, Modified rodnan skin score
© 2026 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2026v18i1.8037 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
The assessment of skin stiffness and thickness plays a critical role in diagnosing and monitoring various dermatologic and connective tissue disorders. Skin thickness reflects the structural integrity, while stiffness provides insights into the bio-mechanical properties of cutaneous tissue. Traditional clinical evaluations relying on palpation or caliper measurements are often subjective and lack reproducibility [1].
Scleroderma, or systemic sclerosis (SSc), is a chronic autoimmune connective tissue disease typified by progressive skin fibrosis due to excessive collagen deposition, associated vasculopathy, and immune dysregulation. This fibrotic skin involvement manifests as increased thickness and stiffness, significantly impacting skin function and patient quality of life [2]. The condition is classified mainly into limited and diffuse cutaneous subtypes, the latter associated with more extensive skin and internal organ involvement. Early and accurate quantification of skin changes is imperative for disease staging, monitoring therapeutic response, and prognostication [3].
Globally, SSc prevalence estimates range widely, with fig. from approximately 7 to 650 cases per million population, influenced by geographic and ethnic factors [4]. Incidence rates worldwide approximate 16.4 per 100,000 person-years [5], illustrating the rarity yet clinical significance of the disease. Indian cohorts predominantly present a younger age of onset and a higher prevalence of diffuse cutaneous involvement compared to Western population [6].
High-frequency ultrasound (HFUS) enables precise, non-invasive visualization of skin layers, quantifying thickness changes reflective of fibrotic progression. Shear Wave Elastography (SWE) assesses biomechanical properties, quantifying stiffness variations correlated with fibrotic activity [7, 8]. This integrated imaging approach enhances diagnostic accuracy, quantifies disease severity, and monitors therapeutic efficacy.
This study aims to quantitatively assess skin thickness and stiffness using high-frequency ultrasound and shear wave elastography in patients with scleroderma compared to healthy controls. We seek to evaluate the diagnostic performance of these imaging modalities, analyze correlations with clinical scores, and establish their utility in early diagnosis and management of scleroderma.
MATERIALS AND METHODS
Study design
This study was designed as a prospective, comparative observational analysis over a 12 mo period at a tertiary hospital in South India. Ethical approval was obtained from the institutional review board, and written informed consent was secured from all participants prior to study enrollment.
Study population
The study comprised adults aged 18–65 years who met the 2013 ACR/EULAR criteria for systemic sclerosis (SSc). Age-and sex-matched healthy controls without any connective tissue or dermatological disorders were recruited.
Case Group: 37 patients diagnosed with systemic sclerosis (both diffuse and limited cutaneous subtypes).
Control Group: 37 healthy volunteers matched by age and sex without any history of autoimmune or skin diseases.
Both groups underwent identical assessments using high-frequency ultrasound and shear wave elastography at standardized anatomical sites, conducted by blinded, experienced operators.
Inclusion criteria
Adults between 18 and 65 y of age.
Diagnosis of SSc based on the 2013 ACR/EULAR criteria.
Both diffuse and limited cutaneous subtypes included.
Willingness to participate and provide informed consent.
Exclusion criteria
Coexisting dermatological, metabolic, or inflammatory conditions affecting skin.
Recent use (within 3 mo) of corticosteroids or immunosuppressive therapies.
Localized scleroderma/morphea rather than systemic.
Pregnancy or lactation.
History of skin ulcers, infections, or trauma in the area to be assessed.
Unwillingness or inability to comply with study protocol.
Assessment tools
High-frequency ultrasound (HFUS): B-mode ultrasonography using a ≥15 MHz linear probe to measure skin thickness at predetermined anatomical sites.
Shear Wave Elastography (SWE): Integrated into the ultrasound system for quantitative stiffness assessment, reported in kilopascals (kPa).
Procedure
Skin thickness and stiffness were measured at standardized sites, including fingers (dorsal mid-phalanx), forearms, and dorsal hands. Each site received three measurements for both modalities, and the mean value was recorded. Assessment was performed by two experienced sonographers blinded to clinical status. The modified Rodnan Skin Score (mRSS) was used to clinically grade skin involvement prior to imaging.
Measurements were performed with the patient at rest in a temperature-controlled room.
Controls underwent identical assessment protocols.
Statistical analysis
Descriptive statistics summarized continuous and categorical variables mean (SD) skin thickness and stiffness between SSc and controls were compared using t-tests or Mann-Whitney U-tests, as appropriate. Correlations between ultrasound-derived measures and mRSS were evaluated by Spearman rank correlation coefficient. ROC curve analyses determined diagnostic performance of each modality. All analyses were conducted with SPSS v25.0, with a p-value<0.05 considered statistically significant.
Table 1: Baseline characteristics of study population
| Parameter | SSc group (n=37) | Control group (n=37) | p-value |
| Age (years) | 45.2±12.6 | 44.1±11.8 | 0.64 |
| Female (%) | 83.8 | 81.1 | 0.77 |
| Disease duration (yrs) | 8.5±4.2 | NA | NA |
| Diffuse SSc (%) | 64.9 | NA | NA |
| Limited SSc (%) | 35.1 | NA | NA |
Table 1 indicates the demographic distribution between groups, showing comparable age and sex, and displaying the percentages of diffuse and limited cutaneous forms in SSc patients.
Table 2: Skin stiffness and thickness by ultrasound (SSc cases vs controls)
| Site | Stiffness (kPa) case | Thickness (mm) case | Stiffness (kPa) control | Thickness (mm) control | p-value |
| Fingers | 49.8 | 1.99 | 18.3 | 1.59 | <0.001 |
| Forearms | 47.6 | 1.85 | 19.2 | 1.53 | <0.001 |
| Dorsum Hands | 45.2 | 1.84 | 17.9 | 1.56 | <0.001 |
Table 2 demonstrates significantly increased skin thickness and stiffness at all measured sites in SSc patients compared to controls, with the highest values seen in fingers and forearms
Table 3: Skin stiffness and thickness by shear wave elastography (SWE)
| Site | Stiffness (kPa) case | Thickness (mm) case | Stiffness (kPa) control | Thickness (mm) control | p-value |
| Fingers | 49.8 | 1.99 | 18.3 | 1.59 | <0.001 |
| Forearms | 47.6 | 1.85 | 19.2 | 1.53 | <0.001 |
| Dorsum Hands | 45.2 | 1.84 | 17.9 | 1.56 | <0.001 |
Table 3 highlights the marked increase in skin stiffness and thickness values in SSc measured using SWE, with statistically significant differences across all sites
Table 4: Correlation of HFUS/SWE with clinical skin score (mRSS)
| Measurement | Spearman’s rho | p-value |
| HFUS Thickness | 0.642 | <0.001 |
| SWE Stiffness | 0.758 | <0.001 |
Table 4 indicates strong positive correlations between both HFUS thickness and SWE stiffness measurements with the modified Rodnan skin score (mRSS), with SWE showing slightly higher correlation strength.
Table 5: ROC Analysis for diagnostic performance
| Modality | AUC | Sensitivity | Specificity | Cut-off Value |
| HFUS Thickness | 0.795 | 82% | 76% | 1.72 mm |
| SWE Stiffness | 0.881 | 90% | 83% | 27.7 kPa |
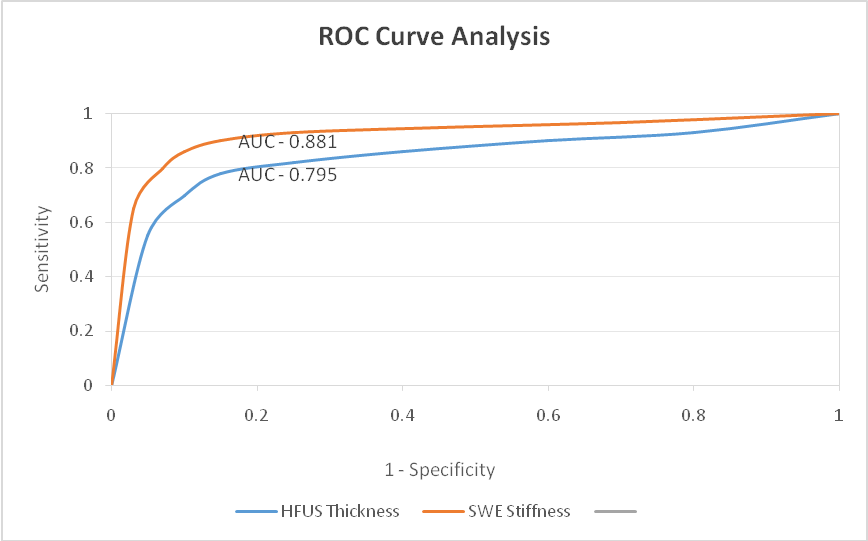
Fig. 1: ROC analysis for diagnostic performance
Table 5 and fig. 1 demonstrates the diagnostic accuracy of both modalities for differentiating SSc skin from normal, with SWE exhibiting the highest area under the curve, sensitivity, and specificity.
DISCUSSION
In the present study, the systemic sclerosis (SSc) patient group had a mean age of 45.2±12.6 y with a female predominance of 83.8%, and a median disease duration of 8.5 y. The diffuse cutaneous subtype accounted for 64.9% of cases, while limited cutaneous SSc was seen in 35.1%. These demographic features closely align with findings from Indian cohorts reported by Ghosh et al. [9], who observed a mean age of 47.5 y, 81% female patients, and similar subtype distribution. Comparable results were reported in Eastern India with a mean age of 29.6 y and 86.9% females, and Jharkhand data showing an 80% female predominance with majority diffuse cutaneous involvement [10].
In our study, patients with systemic sclerosis exhibited a significantly increased skin thickness measured by high-frequency ultrasound across all assessed sites. The mean skin thickness at the fingers was 1.99±0.31 mm, forearms 1.85±0.27 mm, and dorsal hands 1.84±0.26 mm, all markedly higher than in healthy controls (p<0.001). These findings emphasize the role of HFUS as a sensitive tool to detect and quantify fibrotic skin changes characteristic of scleroderma. Wang et al. [11] in his study also reported dermal thickness at the forearm as 1.6138±0.4217 mm (right) and 1.5696±0.3900 mm (left), which again are lower than our SSc cohort’s full-thickness measurements, indicating disease-related thickening evident in our study.
In our study, shear wave elastography (SWE) revealed significantly increased skin stiffness at measured sites in systemic sclerosis patients compared to controls. The mean stiffness values for the fingers, forearms, and dorsal hands were 49.8±12.4 kPa, 47.6±11.8 kPa, and 45.2±11.2 kPa, respectively, compared to 18.3±6.1 kPa, 19.2±6.5 kPa, and 17.9±6.3 kPa in controls, with all differences statistically significant (p<0.001). These findings affirm SWE as a sensitive modality for detecting biomechanical alterations in scleroderma skin, demonstrating marked increases in stiffness correlated with disease pathology. Similarly, Yang et al. [12] demonstrated that shear wave elastography (SWE)-based skin stiffness and high-frequency ultrasound (HFUS)-based skin thickness are effective in distinguishing limited (lcSSc) from diffuse cutaneous systemic sclerosis (dcSSc). Their findings showed significantly higher stiffness values in dcSSc across multiple sites, such as the forearm (median 58.4 kPa) and arm (51 kPa), compared to lcSSc, with strong statistical significance (p<0.001).
Our study showed a strong positive correlation between skin stiffness measured by shear wave elastography and skin thickness measured by high-frequency ultrasound with the modified Rodnan skin score (mRSS), a clinical measure of skin involvement severity in systemic sclerosis. The correlation coefficient for SWE stiffness (r = 0.758, p<0.001) is higher than that for HFUS thickness (r = 0.642, p<0.001), indicating SWE might be a more sensitive indicator of disease severity. These findings concord with Hong et al.[13], where significant differences in shear wave velocity (SWV) and skin thickness sums were noted, and strong associations with clinical scores (r = 0.726 and 0.679) were reported.
SWE demonstrated superior diagnostic accuracy with an area under the curve (AUC) of 0.881 compared to 0.795 for HFUS. Additionally, SWE showed higher sensitivity (90%) and specificity (83%) relative to HFUS (82% sensitivity and 76% specificity). The cut-off values identified (27.7 kPa for SWE stiffness and 1.72 mm for HFUS thickness) provide practical thresholds for clinical application. Yu et al. [14] reported the combined use of HFU and SWE yielded an excellent AUC of 0.980, highlighting synergistic diagnostic potential.
CONCLUSION
This study demonstrated that high-frequency ultrasound (HFU) and shear wave elastography (SWE) are reliable and quantitative tools for assessing skin involvement in systemic sclerosis. Both methods showed significantly increased skin thickness and stiffness in affected patients, correlating strongly with the modified Rodnan skin score (mRSS). The combined use of HFU and SWE provided superior diagnostic accuracy compared to either modality alone, suggesting synergistic benefit. Despite limitations such as a single-center design and small sample size, the findings support ultrasound’s clinical value for diagnosis and monitoring in systemic sclerosis. Standardized protocols and larger multi-center studies are needed to validate and optimize ultrasound's role in routine care.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICTS OF INTERESTS
Declared none
REFERENCES
Lewandowski Z, Dychała E, Pisula Lewandowska A, Danel DP. Comparison of skinfold thickness measured by caliper and ultrasound scanner in normative weight women. Int J Environ Res Public Health. 2022 Dec 4;19(23):16230. doi: 10.3390/ijerph192316230, PMID 36498301.
Son HH, Moon SJ. Pathogenesis of systemic sclerosis: an integrative review of recent advances. J Rheum Dis. 2025 Apr 1;32(2):89-104. doi: 10.4078/jrd.2024.0129, PMID 40134549.
Desai R, Chawla H, Larin K, Assassi S. Methods for objective assessment of skin involvement in systemic sclerosis. Curr Opin Rheumatol. 2023 Nov 1;35(6):301-8. doi: 10.1097/BOR.0000000000000968, PMID 37605869.
Abbot S, Bossingham D, Proudman S, De Costa C, Ho-Huynh A. Risk factors for the development of systemic sclerosis: a systematic review of the literature. Rheumatol Adv Pract. 2018 Oct 11;2(2):rky041. doi: 10.1093/rap/rky041, PMID 31431978.
Fan Y, Bender S, Shi W, Zoz D. Incidence and prevalence of systemic sclerosis and systemic sclerosis with interstitial lung disease in the United States. J Manag Care Spec Pharm. 2020 Dec;26(12):1539-47. doi: 10.18553/jmcp.2020.20136, PMID 32996805.
Philip SS, Janardana R, Shenoy P, Kavadichanda C, Bairwa D, Sircar G. Exploratory clinical subgroup clustering in systemic sclerosis: results from the Indian progressive systemic sclerosis registry. J Scleroderma Relat Disord. 2024;9(1):29-37. doi: 10.1177/23971983231215470, PMID 38333526.
Santiago T, Santos E, Ruaro B, Lepri G, Green L, Wildt M. Ultrasound and elastography in the assessment of skin involvement in systemic sclerosis: a systematic literature review focusing on validation and standardization WSF skin ultrasound group. Semin Arthritis Rheum. 2022 Feb;52:151954. doi: 10.1016/j.semarthrit.2022.151954, PMID 35039184.
Iagnocco A, Kaloudi O, Perella C, Bandinelli F, Riccieri V, Vasile M. Ultrasound elastography assessment of skin involvement in systemic sclerosis: lights and shadows. J Rheumatol. 2010 Aug 1;37(8):1688-91. doi: 10.3899/jrheum.090974, PMID 20551100.
Ghosh S, Tanna D, Telang K, Dhuria S, Gupta R. Clinical and autoantibody profiles of systemic sclerosis patients: a cross-sectional study from North India. Indian J Dermatol Venereol Leprol. 2024;90(4);440-6. doi: 10.25259/IJDVL_901_2022, PMID 37436007.
Ghosh SK, Bandyopadhyay D, Saha I, Barua JK. Mucocutaneous and demographic features of systemic sclerosis: a profile of 46 patients from eastern India. Indian J Dermatol. 2012 May;57(3):201-5. doi: 10.4103/0019-5154.96193, PMID 22707772.
Wang Y, Tian M, Guo R, Du F, Qiu L, Tang Y. Quantification of normal skin thickness using very high-frequency ultrasound: a clinical study in Chinese adults. Quant Imaging Med Surg. 2025 Jun 6;15(6):5218-31. doi: 10.21037/qims-2024-2637, PMID 40606357.
Yang Y, Tang X, Zhong L, Zhang L, Tang Y, Wang Y. Shear wave elastography-based skin assessment system for systemic sclerosis: a supplement or alternative to conventional ultrasound? Quant Imaging Med Surg. 2023 Jul 1;13(7):4405-14. doi: 10.21037/qims-22-1267, PMID 37456300.
Hong DR, Huang CY, Xu ZH. Evaluating skin involvement in systemic sclerosis using high-frequency ultrasound and virtual touch tissue imaging. Ultrasound Med Biol. 2024 Apr;50(4):536-9. doi: 10.1016/j.ultrasmedbio.2023.12.017, PMID 38233292.
Yu S, Peng H, Yang X, Ma S, Yu J, Zuo D. The diagnostic value and clinical relevance of high frequency ultrasound and shear wave elastography in systemic sclerosis: an observational monocentric study. Clin Rheumatol. 2024 Dec;43(12):3759-69. doi: 10.1007/s10067-024-07145-6, PMID 39367267.