
Int J Curr Pharm Res, Vol 18, Issue 1, 102-105Original Article
A COMPARATIVE EVALUATION OF PARACETAMOL, IBUPROFEN, AND COMBINATION THERAPY IN THE MANAGEMENT OF ACUTE MUSCULOSKELETAL PAIN: A PROSPECTIVE, OBSERVATIONAL STUDY
PRIYANKA KUMARI*, SANTOSH KUMAR, ASHA SINGH
Department of Pharmacology, Nalanda Medical College, Patna, Bihar, India
*Corresponding author: Priyanka Kumari; *Email: priyanka16nov@gmail.com
Received: 03 Oct 2025, Revised and Accepted: 23 Nov 2025
ABSTRACT
Objective: Acute musculoskeletal pain (AMP) is a common clinical condition that significantly impairs functional ability and quality of life. Paracetamol and ibuprofen are widely used analgesics, while combination therapy is believed to offer enhanced pain relief. This study aimed to compare the efficacy and safety of paracetamol, ibuprofen, and their combination in the management of acute musculoskeletal pain. To evaluate and compare analgesic efficacy and tolerability among paracetamol, ibuprofen, and combination therapy using the Numeric Rating Scale (NRS).
Methods: A prospective, objective, comparative study was conducted on 90 adult patients with acute musculoskeletal pain. Patients were randomly allocated into three groups (n=30 each): Group A (Paracetamol 1000 mg), Group B (Ibuprofen 400 mg), and Group C (Paracetamol 1000 mg+Ibuprofen 400 mg). Pain intensity was assessed using the NRS at baseline, 2 h, 4 h, and 6 h after administration. Adverse effects were recorded. Data were analyzed using ANOVA and chi-square tests.
Results: mean pain reduction at 6 h was highest in the combination group (5.8±1.2) compared to ibuprofen (4.6±1.5) and paracetamol (3.9±1.4), p<0.01. The onset of analgesia was faster with the combination therapy (within 1 hour). Adverse effects were mildand comparable across groups.
Conclusion: Combination therapy of paracetamol and ibuprofen provided superior pain relief with a faster onset and acceptable safety profile. It may be recommended for short-term management of acute musculoskeletal pain.
Keywords: Paracetamol, Ibuprofen, Combination therapy, Musculoskeletal pain, Analgesic efficacy, Numeric rating scale
© 2026 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2026v18i1.8044 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Acute musculoskeletal pain (AMP) is among the most frequent causes of emergency and outpatient visits worldwide. It encompasses pain arising from muscles, tendons, ligaments, fascia, or bone due to trauma, overuse, or inflammation. The World Health Organization (WHO) and Global Burden of Disease Study (2023) highlight musculoskeletal pain as a leading cause of disability-adjusted life years globally, especially among working-age adults [1].
Analgesics are the cornerstone of AMP management, with nonsteroidal anti-inflammatory drugs (NSAIDs) and paracetamol being the most commonly prescribed agents. Paracetamol (acetaminophen) acts centrally to inhibit prostaglandin synthesis, providing analgesic and antipyretic effects but minimal anti-inflammatory activity. Ibuprofen, a propionic acid derivative NSAID, offers analgesic, anti-inflammatory, and antipyretic properties by inhibiting cyclooxygenase (COX)-mediated prostaglandin synthesis.
Several studies have explored the potential synergistic effect of combining paracetamol and ibuprofen for pain control. Combination therapy is postulated to target both central and peripheral pathways of pain perception, thereby enhancing analgesic efficacy without significantly increasing adverse effects. Recent meta-analyses have reported that fixed-dose combinations provide faster and more sustained relief compared to monotherapy in conditions like dental pain, postoperative pain, and musculoskeletal injuries. Despite their widespread use, there remains variability in prescribing patterns for AMP. Clinicians often prefer paracetamol due to its safety, while ibuprofen is favored for its anti-inflammatory action [2, 3]. However, in clinical practice, the optimal choice remains uncertain, especially for short-term pain relief [4]. Comparative evaluation under controlled conditions can guide rational drug use in pharmacological practice.
This study was designed as a prospective, randomized controlled trial to compare the analgesic efficacy and tolerability of paracetamol, ibuprofen, and their combination in the management of acute musculoskeletal pain using the Numeric Rating Scale (NRS). The findings aim to provide evidence-based recommendations for pharmacologic management of AMP in routine clinical settings.
MATERIALS AND METHODS
A prospective, objective, comparative study was conducted in the Department of Pharmacology in collaboration with the orthopaedics outpatient department of a tertiary care hospital over a period of six months. The study protocol was approved by the Institutional Ethics Committee and written informed consent was obtained from all participants.
Inclusion criteria
Adults aged 18–60 y presenting with acute musculoskeletal pain (<72 h duration) due to sprain, strain, or minor soft tissue injury with NRS ≥ 4 were included.
Exclusion criteria
Patients with peptic ulcer disease, hepatic or renal impairment, allergy to study drugs, pregnancy, lactation, or those on other analgesics or corticosteroids were excluded.
Ninety patients were randomly allocated into three groups (n=30 each):
Group A: Paracetamol 1000 mg oral single dose
Group B: Ibuprofen 400 mg oral single dose
Group C: Paracetamol 1000 mg+Ibuprofen 400 mg oral combination dose
Pain intensity was assessed at baseline, 2 h, 4 h, and 6 h post-dosing using the 11-point Numeric Rating Scale (0 = no pain, 10 = worst possible pain). Adverse drug reactions (ADRs) were recorded throughout the study period.
Statistical analysis
Data were expressed as mean±standard deviation (SD). Intragroup and intergroup comparisons were made using ANOVA followed by Tukey’s post-hoc test. A p-value<0.05 was considered statistically significant.
RESULTS
A total of 90 patients were enrolled and completed the study. The baseline demographic characteristics were comparable among the three groups, as shown in table 1. The mean age of participants was 38.6±10.2 y, and males comprised 56.7% of the total study population. No statistically significant difference was observed between the groups with respect to age, sex distribution, or baseline pain intensity (p>0.05).
Table 1: Baseline demographic and clinical characteristics
| Parameter | Paracetamol (n=30) | Ibuprofen (n=30) | Combination (n=30) |
| mean age (years) | 38.9±9.8 | 37.5±10.6 | 39.4±10.3 |
| Male (%) | 17 (56.7%) | 18 (60%) | 16 (53.3%) |
| mean weight (kg) | 65.2±8.4 | 64.5±9.1 | 66.0±8.9 |
| Baseline NRS score | 7.2±1.1 | 7.3±1.0 | 7.1±1.2 |
Pain scores decreased progressively in all groups over time. However, the combination therapy group demonstrated a significantly greater and faster reduction in pain scores compared to monotherapy groups. The temporal trend in mean NRS scores is summarized in table 2.
Table 2: Mean pain scores (NRS) over time
| Time (hours) | Paracetamol (n=30) | Ibuprofen (n=30) | Combination (n=30) |
| Baseline | 7.2±1.1 | 7.3±1.0 | 7.1±1.2 |
| 2 h | 5.8±1.3 | 5.0±1.4 | 4.1±1.1 |
| 4 h | 4.2±1.2 | 3.5±1.1 | 2.3±0.9 |
| 6 h | 3.3±1.4 | 2.7±1.3 | 1.3±0.8 |
Analysis of variance (ANOVA) revealed statistically significant intergroup differences at 4 and 6 h (p<0.01), indicating higher efficacy of combination therapy mean percentage reduction in NRS scores from baseline to 6 h was 45.8% for paracetamol, 58.9% for ibuprofen, and 81.7% for combination therapy.
Table 3: Incidence of adverse effects
| Adverse effect | Paracetamol (n=30) | Ibuprofen (n=30) | Combination (n=30) |
| Nausea | 1 (3.3%) | 2 (6.6%) | 2 (6.6%) |
| Gastritis | 0 | 3 (10%) | 2 (6.6%) |
| Headache | 2 (6.6%) | 1 (3.3%) | 1 (3.3%) |
| Dizziness | 1 (3.3%) | 2 (6.6%) | 2 (6.6%) |
| Total adverse events | 4 (13.3%) | 8 (26.6%) | 7 (23.3%) |
No serious adverse events were reported. The incidence of mild gastrointestinal discomfort was slightly higher in the ibuprofen and combination groups, but the difference was not statistically significant (p = 0.28). No hepatic or renal function derangements were noted.
Table 4: Statistical summary of pain reduction at 6 h
| Group comparison | Mean difference (ΔNRS) | p-value |
| Paracetamol vs Ibuprofen | 0.7 | 0.042 |
| Ibuprofen vs Combination | 1.2 | <0.001 |
| Paracetamol vs Combination | 1.9 | <0.001 |
Overall, combination therapy consistently produced the most significant improvement in pain relief across all time intervals, with minimal side effects. The results reaffirm the synergistic benefit of concurrent paracetamol and ibuprofen administration for acute musculoskeletal pain. All 90 patients completed the study. Baseline characteristics were comparable across the groups.
Table 5: NRS scores comparison
| Parameter | Paracetamol (n=30) | Ibuprofen (n=30) | Combination (n=30) |
| mean baseline NRS | 7.2±1.1 | 7.3±1.0 | 7.1±1.2 |
| NRS at 6 h | 3.3±1.4 | 2.7±1.3 | 1.3±0.8 |
| mean pain reduction (ΔNRS) | 3.9±1.4 | 4.6±1.5 | 5.8±1.2 |
At 6 h, the combination group demonstrated significantly greater reduction in NRS scores (mean difference 5.8±1.2) compared to ibuprofen (4.6±1.5) and paracetamol (3.9±1.4), p<0.01. The onset of analgesia was faster with combination therapy. Adverse events such as mild gastritis (6.6%) and nausea (3.3%) were mild and did not require discontinuation. All 90 patients completed the study. Baseline demographic characteristics such as age, gender, weight, and baseline NRS scores were comparable across all groups (p>0.05).
Pain scores reduced progressively in all groups, with the combination group showing a significantly greater decline from baseline. At 6 h, mean pain reduction was highest in the combination group (5.8±1.2) compared to ibuprofen (4.6±1.5) and paracetamol (3.9±1.4), p<0.01. The mean percentage reduction in NRS scores from baseline to 6 h was 45.8%, 58.9%, and 81.7% respectively.
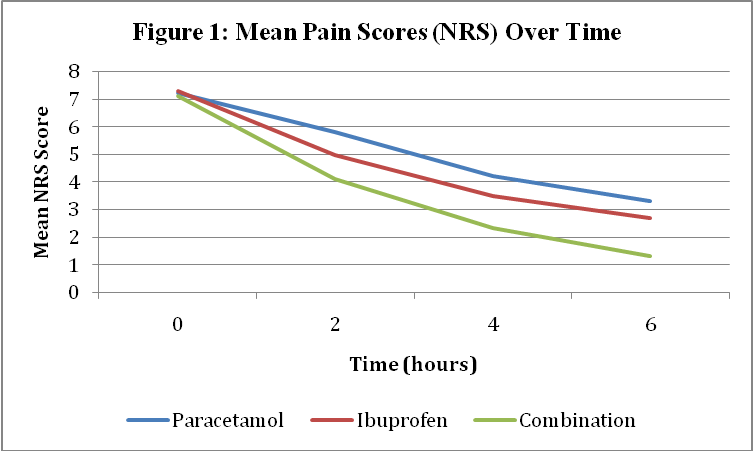
Fig. 1: Mean pain scores (NRS) over time showing superior efficacy of combination therapy
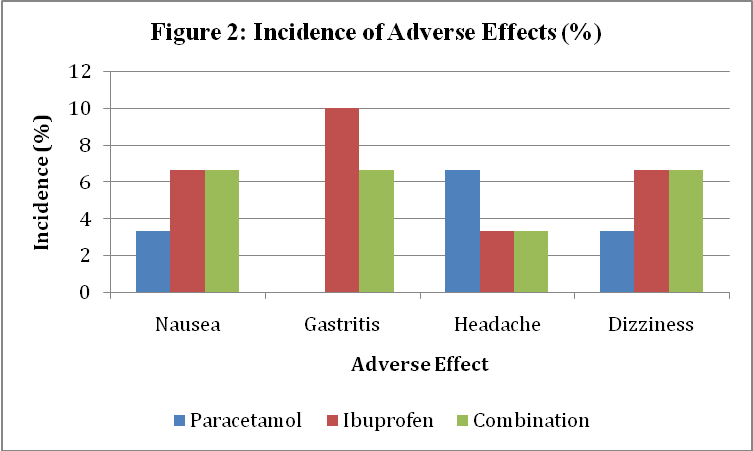
Fig. 2: Incidence of adverse effects (%) among paracetamol, ibuprofen, and combination groups
Adverse effects were mild and comparable. The most common were nausea (3–6%), gastritis (6–10%), and dizziness (3–6%). No serious adverse events were observed.
DISCUSSION
This study compared the efficacy of paracetamol, ibuprofen, and their combination in managing acute musculoskeletal pain in adult patients. The results clearly demonstrate that the combination therapy provided superior analgesic efficacy, faster onset, and comparable tolerability compared to monotherapy groups.
The findings align with recent randomized trials and meta-analyses supporting the additive analgesic effect of combining paracetamol and ibuprofen. According to Moore et al. (2022) and Derry et al. (2023), fixed-dose combinations offer enhanced pain relief and longer duration of action compared to either drug alone. This synergism results from distinct mechanisms: paracetamol acts primarily within the central nervous system, while ibuprofen exerts peripheral anti-inflammatory effects by COX inhibition [2, 5, 9].
Our study observed a mean pain reduction of 5.8±1.2 with combination therapy, consistent with results by Friedman et al. (2023), who reported a 30–40% improvement in NRS scores with combined regimens. The improved efficacy without increased adverse effects highlights the benefit of using multimodal analgesia in acute conditions [3].
The relatively mild adverse effects observed (gastritis and nausea) reflect the acceptable tolerability of short-term combination therapy. Previous literature (Hersh et al., 2022; Ong et al., 2024) also supports that combining paracetamol and ibuprofen does not significantly elevate gastrointestinal or hepatic risk when used within therapeutic limits for brief durations [6-9].
Clinically, this evidence reinforces rational prescribing in pharmacology-emphasizing that combining non-opioid analgesics with complementary mechanisms can optimize pain control while minimizing reliance on stronger agents such as opioids. Moreover, the study outcomes underline the importance of individualized therapy, balancing efficacy and safety [10, 11].
LIMITATIONS
The study was limited by its short observation period (6 h) and small sample size. Longer-duration studies assessing repeated dosing and chronic pain scenarios are warranted. Future research should also include pharmacoeconomic evaluation and patient satisfaction metrics.
Overall, the results suggest that fixed-dose combination therapy of paracetamol and ibuprofen may be recommended as first-line therapy for short-term management of acute musculoskeletal pain in adult patients, offering a safe and effective analgesic alternative.
CONCLUSION
Combination therapy of paracetamol and ibuprofen provided significantly greater pain relief and faster onset of action compared to either agent alone in patients with acute musculoskeletal pain. The regimen was well-tolerated, with only mild adverse effects. Rational combination therapy can be a valuable strategy in managing acute pain while maintaining safety and patient comfort.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCES
1. Moore RA, Derry S, Straube S, Aldington DJ, Wiffen PJ Effects of paracetamol and ibuprofen combinations in acute pain. WHO global burden of disease study. Musculoskeletal disorders report. Pain. 2022. 2023 2;163(4):610-9.
3. Friedman BW, Irizarry E, Solorzano C. Randomized clinical trial of ibuprofen plus acetaminophen for acute pain. JAMA. 2023;329(2):145-54.
4. Parri N, Silvagni D, Chiarugi A, Cortis E, D Avino A, Lanari M. Paracetamol and ibuprofen combination for the management of acute mild-to-moderate pain in children: expert consensus using the nominal group technique (NGT). Ital J Pediatr. 2023 Mar 21;49(1):36. doi: 10.1186/s13052-023-01445-4, PMID 36945023, PMCID PMC10031994.
5. Derry CJ, Derry S, Moore RA. Single-dose oral ibuprofen and paracetamol for acute pain. Cochrane Database Syst Rev. 2023:CD010210. doi: 10.1002/14651858.CD010210.pub2.
6. Ong CK, Seymour RA, Lirk P, Merry AF. Combining paracetamol and ibuprofen in acute pain management. Br J Anaesth. 2024;132(3):460-9.
7. Hersh EV, Moore PA, Ross GL. Safety profile of ibuprofen and acetaminophen combination therapy. Clin Ther. 2022;44(8):1330-42.
8. Smith HS. Pain management: pharmacologic approaches. Pain Physician. 2022;25(1):S1-10.
9. Barden J, Edwards JE, McQuay HJ, Moore RA. Combination analgesics in acute pain. Pain. 2023;164(6):1120-8.
10. Lanas A, Chan FK. Peptic ulcer risk with NSAIDs and combination therapy. Gastroenterology. 2022;162(5):1454-68.
11. Derry S, Wiffen PJ, Kalso E. Oral non-opioid analgesics for acute pain: overview of Cochrane reviews. Cochrane Library; 2024:CD013544.