
Int J Curr Pharm Res, Vol 18, Issue 1, 85-87Original Article
SERUM FERRITIN LEVEL IN CHILDREN WITH 𝛽-THALASSEMIA MAJOR: A HOSPITAL-BASED PILOT STUDY
DIVYA GUPTA1*, JAGDAMBA DIXIT2
1Department of Biochemistry, People’s College of Medical Sciences, and Research, (PCMS and RC), Bhopal-462037, India. 2Department of Pediatrics, People’s College of Medical Sciences and Research (PCMS and RC), Bhopal-462037, India
*Corresponding author: Divya Gupta; *Email: divyaaiims2018@gmail.com
Received: 06 Oct 2025, Revised and Accepted: 26 Nov 2025
ABSTRACT
Objective: To study the serum ferritin level in children with 𝛽-TM patients.
Methods: Clinico-pathological details of 𝛽-TM patient’s were entered into a Microsoft Excel and exported to SPSS version 21 (IBM SPSS® software, Chicago, US). P value<0.05 was considered as statistically significant.
Results: Significant correlation between serum ferritin value (P-value 0.001) (mean 1868.67and SD value 1427.68) and number of blood transfusion (mean 67.77 and SD value 66.88) have been observed. Increased number of blood transfusion is associated with increased serum ferritin value (P-value 0.001 and correlation coefficient 0.536**), which represent the iron overload.
Conclusion: Regular monitoring of serum ferritin, and other biochemical parameters will improve the health of 𝛽-TM patients. Higher numbers of study samples are needed to validate the result of 𝛽-TM patients. Significant correlation has been observed in serum ferritin which shows the iron overload in 𝛽-TM patients. Furthermore, we need to study on larger sample size for iron overload in 𝛽-TM patients.
Keywords: 𝛽-Thalassemia, Ferritin, Iron overload, Blood transfusion, BMI
© 2026 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2026v18i1.58164 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
𝛽-Thalassemia major (𝛽-TM) is a monogenic disorder which affects an autosomal recessive manner. Globally, it is estimated that 300,000 to 400,000 babies are born with hemoglobinopathies, with approximately 23,000 cases per year affected from thalassemia major [1]. In India, 𝛽-thalassemia is prevalent across the country, and around 10,000–12,000 𝛽-TM infants are born annually. According to national sickle cell anemia mission a higher frequency has been observed in Indian communities [2].
In the 𝛽-TM patients, damage of erythropoiesis requires lifelong repeated blood transfusions (BT’s) to maintain the hemoglobin (Hb) levels above 9-10.5 g/dl. Due to frequent BT’s cause iron overload and hemosiderosis, which are toxic to the 𝛽-TM patients.
𝛽-TM patients are still experience a range of problems, particularly in relation to their growth, development, malnutrition, transfusion-transmitted infections, tissue damage which affect the liver, heart, and endocrine system and also contribute to the morbidity and mortality [3-5]. The management strategies of thalassemia include: transfusions, chelation agents against iron overload, hydroxyurea, and splenectomy, stimulation of foetal Hb synthesis, and bone marrow/hematopoietic stem cell transplantation [6, 7].
Growth retardation in patients with 𝛽-TM is multifactorial, nutritional imbalance, endocrine abnormality and side effects of chelation therapy. Therefore aim of the study was to analyze the serum ferritin level in children with 𝛽-TM patients.
MATERIALS AND METHODS
Patients and clinical examination
The study was approved by the Institutional Ethics Committee, study done in the Department of Biochemistry, Department of Pediatrics, of the institution. 𝛽-TM patients aged 06 mo to 14 y (6 mo-168 mo), who underwent routine BT and received iron chelation treatment at the institute, were enrolled in the study. Total 35 patient’s samples were chosen for a hospital-based pilot study and all study participants received a standard clinical examination by a pediatrician.
Diagnosis of 𝛽-TM patient’s was confirmed as per their Hb electrophoresis data (HPLC) register under regular BT program in the institute, were included for the study. The study subjects with following criteria excluded from the study; bone marrow transplanted patients, age less than six months and more than 14 y or 168 mo during the study period, HIV infected patients, taking high-dose steroids for two weeks or more and with any other chronic illness such as tuberculosis, cancer, or any other inflammatory bone/joint disorder. The subjects were enrolled in the study underwent routine BTs and received iron chelation treatment at the institute. Serum ferritin value, number of BT and patient’s related clinical information taken from record sheet/patients card at the time of counseling.
Statistical analysis
Clinico-pathological details 𝛽-TM patient’s were entered into a Microsoft Excel and exported to SPSS version 21 (IBM SPSS® software, Chicago, US). The data obtained after counseling from 𝛽-TM patients were subjected to descriptive analysis. The data was not normally distributed; hence non-parametric tests were used for analysis. Bivariate correlation between two variables was analyzed by Spearman-rank’s correlation test. To determine the independent predictor logistic regression analysis was performed and p-value<0.05 considered as statistically significant.
RESULTS
A total of 35 𝛽-TM patients (60%; 22 males and 40%; 13 females), aged 0.6-14 y (6 mo-168 mo) as per the inclusion and exclusion criteria mentioned in the methodology section. The mean age of 𝛽-TM patients was 86.17±47.63 mo (13-156 mo). Based on the age, the patients were categorized into three groups i. e. Group I (N =13, 9M/4F), 0.6-60 mo; Group II (N =14, 9M/5F), 61-120 mo and Group III (N =8, 4M/4F), 121-156 mo. First Hb, first BT and available serum ferritin value of the 𝛽-TM patients are shown in table 1, 2, 3 and 4, respectively.
At the time of diagnosis made calculated mean value of the age, first BT, pre-transfusion Hb level were 12.86 mo, 12.22 mo, 5.5 mg/dl, respectively. The mean Hb value at the time of study enrollment 7.4 mg/dl showed in table 1.
Table 1: Shows the mean values of age, Hb, BT and serum ferritin in the 𝛽-TM patients
| Biochemical parameters | Mean value | Range | SD | |
| Min. | Max. | |||
| Age in months | 86.17 | 13 mo | 156 mo | 47.63 |
| First BT Age (months) | 12.21 | 1 mo | 46 mo | 11.90 |
| Hb value before first BT | 5.55 | 2.3 | 8.9 | 1.45 |
| Hb value current available | 7.40 | 2.4 | 11.0 | 1.65 |
| Total no of BT | 67.77 | 1.00 | 360.00 | 66.88 |
| Serum ferritin ng/ml | 1868.67 | 150.00 | 6583.00 | 1427.68 |
https://www.calculator.net/standard-deviation-calculator.html
In our study 62.85% male and 37.14% were female patients were recruited or enrolled for study. In which male patients had 73.27 mean value for available BT value and 58.46 numbers in female BT value and when we correlate the number and ferritin value we found that 22 male patients showed the mean of serum ferritin value 1876.77 in comparison of 13 female patients showed ferritin value 1854.97 ng/ml, indicate that female patients had high ferritin value even though they were in less numbers in comparison of male 𝛽-TM patients table 2.
Table 2: Shows the mean values of age, Hb, BT and serum ferritin in male and female 𝛽-TM patients
| Anthropometrics parameters | Male (22) 62.85% | Mean | SD | Female (13) 37.14% | Mean | SD |
| Age in months | 1803 | 81.95 | 46.93 | 1213 | 93.30 | 49.86 |
| First BT Age (months) | 282 | 12.81 | 12.61 | 145.5 | 11.19 | 11.03 |
| Hb value before first BT | 127.7 | 5.80 | 1.37 | 65.9 | 5.12 | 1.53 |
| Hb value current available | 167.4 | 7.60 | 1.82 | 91.8 | 7.06 | 1.31 |
| Available no of BT | 1612 | 73.27 | 79.24 | 760 | 58.46 | 39.21 |
| Available Ferritin Value | 41289 | 1876.77 | 1496.16 | 24114.64 | 1854.97 | 1362.85 |
Serum ferritin value
All the patients recruited in the study had iron overload as measured by serum ferritin levels, data recorded from the patient’s data card shown in table 1. Out of 35 patients 13 (42.8%), 11 (34.2%) and 11 (22.8%) exhibited severe, moderate and mild iron overload, respectively. After the analysis of the data on gender basis we found that, 50% frequencies of the male patients were reported in severe condition, 46.1% female showed in moderate condition (>1000 ng/ml) and in mild condition both male and female patients showed equal iron overload. On the basis of patients age we have reported that Group II, 61-120 mo showed the 57.1% ferritin value recorded in the patients of severe condition (>2000 ng/ml) and Group III, 121-156 mo 37.5%, 50%, 12.5% in Severe>2000, Moderate>1000 and Mild<1000 condition respectively in table 3.
Table 3: Shows the serum ferritin levels in the 𝛽-TM patients
𝛽-TM 35 patients-male 22 (60.0%); female 13 (40.0%) Group I-13; Group II-14; Group III-08 |
Serum ferritin ng/ml | ||
| Mild<1000 | Moderate>1000 | Severe>2000 | |
| 11 (22.8%) | 11 (34.2%) | 13 (42.8%) | |
| Gender | M (N =22) | 6 (22.7%) | 8 (27.2%) |
| F(N=13) | 5 (23.0%) | 3 (46.1%) | |
| Age (Months) | Group I | 05 (38.4%) | 04 (30.7%) |
| Group II | 02 (14.2%) | 04 (28.5%) | |
| Group III | 01 (12.5%) | 04 (50%) | |
§Group I, 6-60 mo; Group II, 61-120 mo; Group III, 121-156 mo; M, Male; F, Female. *Vincenzo De Sanctis et al., (2016) [8].
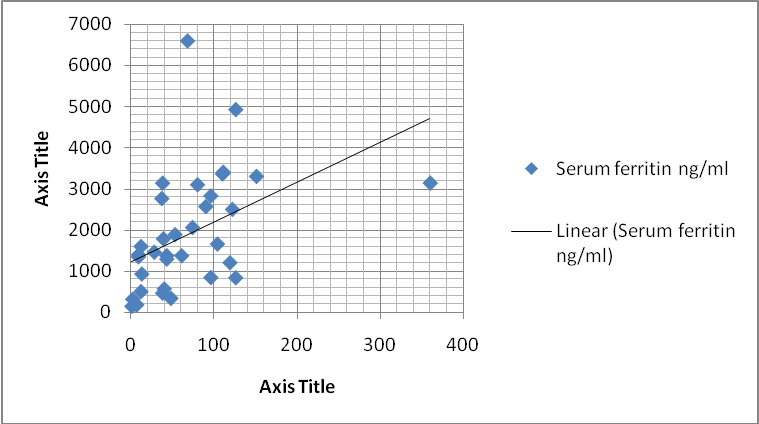
Fig. 1: Shows the line diagram of available serum ferritin value and available number of BT of the 𝛽-TM patients
Table 4: Shows the Pearson correlation and p-value
| Parameters | Correlation | Pearson correlation | Sig. (2-tailed) |
| Ferritin | Total BT number | 0.525** | 0.001 |
| Non-parametric Spearman-rank correlation test | |||
| Parameters | Correlation | Correlation coefficient (rho/) | Sig. (2-tailed) |
| Ferritin | Total BT number | 0.536** | 0.001 |
∗Blood transfusion (BT).
Line diagram of serum ferritin and number of BT shows the significant correlation. Increased number of BT showed the increased serum ferritin value fig. 1.
We also applied the Pearson Correlation in serum ferritin value and number of BT, Pearson Correlation 0.525** with significant p-value 0.001, and non-parametric Spearman-rank correlation test showed that rho/〉=0.536**, p-value 0.001 showed in table 4.
DISCUSSION
𝛽-TM patients encountering difficulties, especially in growth, development, malnutrition, transfusion-transmitted infections, tissue damage, which affect the liver, heart, and endocrine system and also contribute to the morbidity and mortality. Increased number of BT is a significant cause of hepatic iron overload in transfusion-dependent β-TM patients, and iron chelation therapy leads to significant improvement for β-TM patients.
Iron overload leads to the range of complications including cardiac disease, pulmonary hypertension, liver disease, musculoskeletal disorder, chronic pain, and psychiatric disorders [9] and also leading cause of mortality in beta-thalassemia major patients. Endocrine glands are in particular reactive to iron deposits; common endocrine complications of 𝛽-TM are short stature, hypogonadotropic, delayed puberty, impaired glucose tolerance, hypothyroidism, hypoparathyroidism, and diabetes mellitus. Complications may take place in non-endocrine organs, including heart, kidneys, bones, eyes, and other organs [1, 10]. Our study would generate preliminary data which would form the base for studies having larger sample sizes. Furthermore, multicentre studies with large sample size are required.
CONCLUSION
𝛽-TM patients have markedly deranged biochemical profile. Regular monitoring of serum ferritin and other biochemical parameters will improve the health of 𝛽-TM patients. Our study has certain limitations, including a relatively small sample size. Higher numbers of study samples are needed to validate the result of 𝛽-TM patients. Significant correlation has been observed in serum ferritin which shows the iron overload in 𝛽-TM patients.
ACKNOWLEDGEMENT
We acknowledge our appreciation to all 𝛽-TM patients for the participation in the study. Author thanks and acknowledges the support from the institute and collaborating departments such as Department of Biochemistry, Department of Pediatrics
FUNDING
The research work funded by the “Management Cell of PCMS and RC, Bhopal” Grant No. PCMS and RC/OD/PS/23/1062 for the project entitled “Assessment of Biochemical parameters of serum calcium, phosphate, vitamin D, ferritin and thyroid profile in 𝛽-Thalassemia Major patients: A Hospital based Pilot study from Central India.” Divya Gupta has received research support from “Management Cell of PCMS and RC”, Bhopal.
Ethics approval and consent to participate
This study has been approved by Institutional Human Ethics Committee.
Consent for publication
Done as per ethical approval
AUTHORS CONTRIBUTIONS
Divya Gupta Ph. D., was involved in study concepts, design, and collection of samples, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing and review.
CONFLICT OF INTERESTS
The authors declare no conflict of interest.
REFERENCES
De Sanctis V, Soliman AT, Elsedfy H, Skordis N, Kattamis C, Angastiniotis M. Growth and endocrine disorders in thalassemia: the international network on endocrine complications in thalassemia (I-CET) position statement and guidelines. Indian J Endocrinol Metab. 2013;17(1):8-18. doi: 10.4103/2230-8210.107808, PMID 23776848.
Mohanty D, Colah RB, Gorakshakar AC, Patel RZ, Master DC, Mahanta J. Prevalence of β-thalassemia and other haemoglobinopathies in six cities in India: a multicentre study. J Community Genet. 2013;4(1):33-42. doi: 10.1007/s12687-012-0114-0, PMID 23086467.
Kattamis A, Forni GL, Aydinok Y, Viprakasit V. Changing patterns in the epidemiology of β-thalassemia. Eur J Haematol. 2020;105(6):692-703. doi: 10.1111/ejh.13512, PMID 32886826.
Baird DC, Batten SH, Sparks SK. Alpha and beta-thalassemia: rapid evidence review. Am Fam Physician. 2022;105(3):272-80. PMID 35289581.
Ali S, Mumtaz S, Shakir HA, Khan M, Tahir HM, Mumtaz S. Current status of beta-thalassemia and its treatment strategies. Mol Genet Genomic Med. 2021;9(12):e1788. doi: 10.1002/mgg3.1788, PMID 34738740.
Rattananon P, Anurathapan U, Bhukhai K, Hongeng S. The future of gene therapy for transfusion-dependent beta-thalassemia: the power of the lentiviral vector for genetically modified hematopoietic stem cells. Front Pharmacol. 2021;12:730873. doi: 10.3389/fphar.2021.730873, PMID 34658870.
Tang CH, Furnback W, Wang BC, Tang J, Tang D, Lu MY. Relationship between transfusion burden, healthcare resource utilization and complications in patients with beta-thalassemia in Taiwan: a real-world analysis. Transfusion. 2021;61(10):2906-17. doi: 10.1111/trf.16636, PMID 34505291.
De Sanctis V, Soliman AT, Elsedfy H, Soliman NA, Soliman R, El Kholy M. Dysmenorrhea in adolescents and young adults: a review in different country. Acta Biomed. 2016 Jan 16;87(3):233-46. PMID 28112688, PMCID PMC10521891.
Baird DC, Batten SH, Sparks SK. Alpha and beta-thalassemia: rapid evidence review. Am Fam Physician. 2022;105(3):272-80. PMID 35289581.
Taher AT, Saliba AN. Iron overload in thalassemia: different organs at different rates. Hematology Am Soc Hematol Educ Program. 2017;2017(1):265-71. doi: 10.1182/asheducation-2017.1.265, PMID 29222265.