
Int J Curr Pharm Res, Vol 18, Issue 2, 106-111Original Article
COMPARATIVE STUDY OF FNAC AND CELL BLOCK WITH COMBINED RESULT OF BOTH IN DIAGNOSIS OF BREAST LESIONS
KHUSHBOO SHUKLA, SWALAHA SADAF SIDDIQUE*, PRINCE LOKWANI, W. K. RAUT
Department of Pathology, Peoples College of Medical Science and Research Centre, Bhopal (M. P.), India
*Corresponding author: Swalaha Sadaf Siddique; *Email: inaya.sadaf08@gmail.com
Received: 15 Nov 2025, Revised and Accepted: 03 Jan 2026
ABSTRACT
Objective: Breast lesions, ranging from benign to malignant, are common in clinical practice, cancer in breast being a major health issue in India. FNAC is widely used for diagnosis but has limitations that the cell block technique can address by preserving tissue architecture. This study compares the diagnostic performance of FNAC, cell block, and their combined use.
Method: A prospective study involved thirty-two female patients with palpable breast lump. Both cytology smears and cell block preparation has been performed from fine needle aspiration (FNAC) material and compare it with histopathology as the gold standard. Diagnostic metrics were evaluated for each method.
Results: FNAC identified most of benign and malignant cases. Cell block provided additional information, improving the ability to differentiate between benign and malignant lesions. The combined approach offered the most comprehensive diagnostic results. FNAC is effective but may struggle with atypical or suspicious lesions. The cell block provides better tissue architecture and clarity, which is particularly useful in difficult cases. The combination of both methods improves the diagnostic process, helping reduce the need for invasive procedures.
Conclusion: Combining FNAC with the cell block technique significantly improves the ability to diagnose breast lesions accurately. This approach should be considered for enhanced clinical decision-making and patient management.
Keywords: Breast lesions, FNAC, Cell block, Diagnostic accuracy, Invasive ductal carcinoma, Benign lesions, Malignant lesions
© 2026 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2026v18i2.8074 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Breast lesions represent a wide spectrum of pathological conditions, ranging from benign proliferative disorders to malignant neoplasms, and are among the most common clinical presentations encountered in women’s health care. The diversity of breast lesions includes fibrocystic disease, fibroadenoma, mastitis, galactocele, fat necrosis, and various forms of carcinoma, each with distinct clinical and pathological features [1]. The peak incidence of both benign and malignant breast lesions is observed in the fourth and fifth decades of life, highlighting the importance of vigilant screening and diagnostic strategies in this age group [1].
In India, breast cancer has emerged as a significant public health challenge, constituting approximately 26.6% of all female cancers [2, 3]. The incidence rate of breast cancer in Indian women is 26.6 per 100,000, with a mortality rate of 13.7 per 100,000, reflecting both the increasing prevalence and the need for improved early detection and management [2]. These statistics underscore the necessity for efficient, accurate, and minimally invasive diagnostic modalities that can facilitate early diagnosis and guide appropriate management.
Fine Needle Aspiration Cytology (FNAC) has become a cornerstone in the initial evaluation of palpable breast masses due to its minimally invasive nature, cost-effectiveness, high reliability, and low complication rates [4]. FNAC is widely recognized for its ability to provide rapid preliminary diagnosis and can be easily repeated, making it an invaluable tool in both resource-rich and resource-limited settings [5, 6]. The technique involves aspirating cells from the breast lesion, which are then examined cytologically to categorize the lesion into one of several diagnostic categories: inadequate (Category I), benign (Category II), atypical (Category III), suspicious for malignancy (Category IV), or positive for malignancy (Category V).
Despite its advantages, FNAC alone has certain limitations. In some cases, the cytological material obtained may be insufficient for a conclusive diagnosis, particularly when architectural features or additional molecular studies are required. The cell block technique has emerged as an important adjunct to FNAC, addressing many of these limitations. The cell block method involves processing the residual aspirated material into a paraffin-embedded block, which can be sectioned and stained similarly to histological specimens. This approach allows for the preservation of tissue architecture, enabling the assessment of features that may not be discernible on conventional FNAC smears [5]. Moreover, cell block preparations facilitate the application of immunohistochemistry (IHC) and molecular studies such as fluorescence in situ hybridization (FISH), Chromogenic In Situ Hybridization (CISH), and Polymerase Chain Reaction (PCR), which are essential for the accurate subtyping and prognostication of breast lesions [6].
The combined use of FNAC and cell block has been shown to significantly enhance diagnostic accuracy. Studies have demonstrated that while FNAC alone provides valuable cytological information, the addition of cell block allows for a more comprehensive evaluation, particularly in cases with granulomatous lesions, atypical proliferations, or suspicious features [5, 7]. For instance, Ashwinkumar et al. reported that the diagnostic accuracy of FNAC alone was 81.85%, while cell block alone achieved 79.25%. Notably, the combined approach increased accuracy to 87.40%, underscoring the complementary nature of these techniques [7]. Similarly, Raafat et al. and Patel et al. found that cell block diagnosis had a sensitivity of 94% and specificity of 98%, and that the combined utility of FNAC and cell block yielded the best results for both benign and malignant lesions [8].
In clinical practice, the cell block technique is particularly valuable for cases where FNAC smears are inadequate or equivocal, as well as for the preservation of sample material for ancillary testing, including CBNAAT (Cartridge-Based Nucleic Acid Amplification Test) in granulomatous lesions, and for immunohistochemical analysis in categories III, IV, and V lesions. The ability to perform IHC and molecular studies on cell block material is crucial for further diagnosis and precise categorization, especially in the era of personalized medicine [9, 10].
Given these advantages, the present study aims to compare the diagnostic utility of FNAC, cell block, and their combined use in the evaluation of breast lesions. By systematically analyzing the strengths and limitations of each technique, as well as their synergistic potential, this research seeks to provide evidence-based recommendations for optimizing the diagnostic approach to breast lesions in clinical practice. Ultimately, the goal is to enhance diagnostic accuracy, facilitate timely and appropriate patient management, and contribute to improved outcomes for individuals affected by breast pathology.
MATERIALS AND METHODS
Study design
This study was a prospective cross-sectional investigation conducted over a period of nine months at the Department of Pathology, People's College of Medical Sciences and Research Centre, Bhopal, Madhya Pradesh, India. The primary objective was to compare the diagnostic efficacy of Fine Needle Aspiration Cytology (FNAC) and the cell block technique in diagnosing breast lesions, both individually and in combination. By employing these methods, the study sought to provide a comprehensive analysis of their diagnostic accuracy and the potential improvement when both techniques were used together.
Study population
The study involved a total of 32 female patients who presented with palpable breast lesions. These patients were referred to the pathology department for FNAC based on their clinical presentation. Inclusion criteria were adult females with palpable breast masses, irrespective of the type of lesion (benign or suspected malignant), and those who provided written informed consent for participation. Exclusion criteria consisted of patients with non-palpable lesions or those whose lesions were inaccessible for FNAC. Additionally, patients with a prior history of breast surgery or breast cancer treatments were excluded from the study, as were those unwilling to provide consent.
Clinical examination
Before undergoing FNAC and cell block preparation, each patient underwent a thorough clinical examination. A detailed medical history was taken, including the duration of the breast mass, symptoms such as pain or discharge, and any family history of breast cancer. A local physical examination was performed to assess the size, location, and consistency of the lesion, along with any associated signs such as tenderness or changes in the size of the mass. This examination helped determine the approach for FNAC sampling and was essential for categorizing lesions based on their clinical presentation.
FNAC (Fine needle aspiration cytology)
FNAC was performed under aseptic conditions by an experienced pathologist or clinician. The lesion was first identified through palpation and marked for aspiration. The procedure involved cleaning the skin with 70% isopropyl alcohol, followed by the insertion of a 22–23-gauge needle into the lesion. The aspirate was collected using a syringe attached to the needle, and multiple passes were made to ensure adequate material was obtained. At least two alcohol-fixed smears and three air-dried smears were prepared from the aspirate, which were then stained with Papanicolaou stain and Giemsa stain, respectively. These smears were examined microscopically to assess the cytological characteristics of the lesion. The FNAC results were categorized into five diagnostic groups, including Category I (Inadequate), Category II (Benign), Category III (Atypical), Category IV (Suspicious of malignancy), and Category V (Malignant). This categorization was based on cytological features such as cellularity, cell arrangement, and the presence of malignant cells.
Cell block preparation
In addition to FNAC, a portion of the aspirated material was used for cell block preparation, which provides better tissue architecture preservation. After aspirating the lesion, the remaining material was immediately fixed in 10% formalin to preserve the cellular components. The material was then centrifuged to form a pellet. The pellet was embedded in paraffin wax, and thin sections of approximately 5 microns were cut using a microtome. These sections were then mounted onto glass slides and stained with Hematoxylin and Eosin (HandE) for histopathological examination. The cell block technique allowed for a more detailed evaluation of the lesion’s tissue architecture, which is crucial for distinguishing between benign and malignant lesions. The cell block material also allowed for the potential use of immunohistochemistry (IHC) and molecular studies such as Polymerase Chain Reaction (PCR) and fluorescence in situ hybridization (FISH), which were employed in cases where further analysis was needed to refine the diagnosis histopathological.
Correlation
For patients who underwent surgical excision of the breast lesion, the histopathological examination of excised tissue was performed as the gold standard for diagnosis. The results from histopathology were compared with the diagnoses from FNAC and cell block preparations. This comparison helped to determine the diagnostic accuracy of both techniques, providing a benchmark for their effectiveness in diagnosing breast lesions.
Data collection and analysis
Data were collected for each patient, including demographic information, lesion characteristics (size, location, consistency), and diagnostic results from both FNAC and cell block preparations. The FNAC results were classified into five diagnostic categories, and cell block results were analyzed to assess their contribution to the diagnosis. Additionally, the final histopathological diagnosis was used to validate the results of FNAC and cell block. These measures were calculated to compare the performance of FNAC and cell block techniques and to determine whether the combined use of both methods improved diagnostic accuracy.
Statistical analysis
Data analysis was performed using JASP. Descriptive statistics, including frequency and percentage distributions, were used to summarize patient characteristics and lesion types. Diagnostic accuracy was evaluated by calculating the sensitivity, specificity, and predictive values for FNAC, cell block, and their combination. A comparative analysis was conducted to assess the improvement in diagnostic accuracy when both FNAC and cell block were used together. This analysis provided insight into how the combined approach affected the diagnostic outcomes compared to using either technique independently.
Ethical considerations
Ethical considerations were of paramount importance throughout this study. The study protocol was reviewed and approved by the Institutional Ethics Committee of People's College of Medical Sciences and Research Centre, ensuring compliance with ethical standards in medical research. Informed consent was obtained from all participants before any procedure was performed. The patients were fully informed about the purpose of the study, the procedures involved (including FNAC and cell block), and the potential risks, which were minimal but included discomfort and a small risk of complications such as infection or hematoma. The participants were assured that their participation was voluntary, and they could withdraw from the study at any time without affecting their ongoing medical care.
Confidentiality was strictly maintained; with patient identifiers removed from all data collected.
RESULTS
Study population and lesion characteristics
The study included 32 female patients, all presenting with palpable breast lesions, of whom 30 patients were eligible for complete analysis. The ages of the patients ranged from 20 to 70 years, with most patients (approximately 70%) falling within the 30 to 50-year age group. The most common presenting symptom was the presence of a painless mass, which was detected during routine breast self-examination or clinical screening. In terms of lesion types, 22 patients (73%) had benign breast lesions, and 8 patients (27%) were diagnosed with malignant lesions after histopathological confirmation.
Among the benign lesions, fibroadenomas were the most common, making up 12 cases (40%) of the total sample. Other benign lesions included gynecomastia (1 case), fat necrosis (2 cases), and galactocele (2 cases). Invasive ductal carcinoma, malignant lesions, accounted for 8 cases (27%), confirmation with histopathological supporting the FNAC and cell block diagnoses. This distribution reflects the typical epidemiology of breast lesions in India, with a higher incidence of benign lesions compared to malignant ones, especially in younger women.
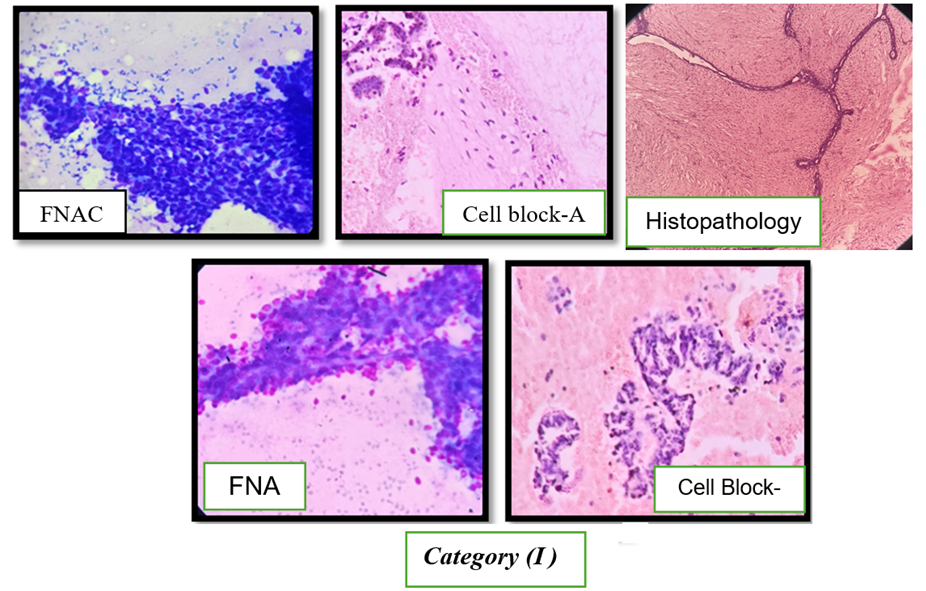
Fig. 1: Cytological and histopathological features of fibroadenoma of the breast, Fine-needle aspiration cytology (FNAC) smears show high cellularity with cohesive sheets and branching clusters of benign ductal epithelial cells admixed with bare bipolar nuclei, consistent with fibroadenoma (upper left and lower left). Cell block preparation (Cell Block-A) demonstrates stromal fragments composed of spindle-shaped cells within a fibromyxoid background along with epithelial components (upper middle). Cell Block-B highlights well-preserved epithelial cell clusters arranged in cohesive patterns without cytological atypia (lower middle). Corresponding histopathology (right panel) reveals characteristic intracanalicular and pericanalicular growth patterns of fibroadenoma, confirming a benign breast lesion (Category II)
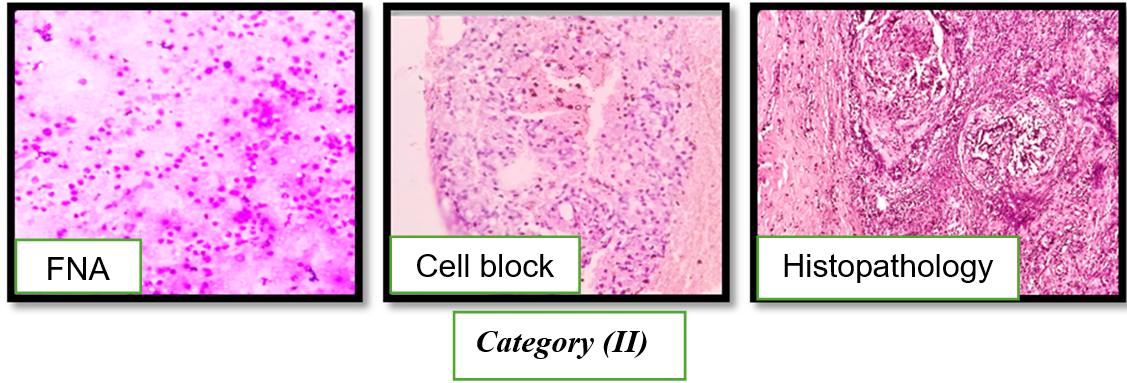
Fig. 2: Cytological, cell block, and histopathological correlation in mastitis of the breast (Category II)
Fine-needle aspiration cytology (FNAC) smears reveal numerous polymorphs and histiocytes and few benign ductal epithelial cells. Cell block preparation shows demonstrates clusters of polymorphs and lympho-histiocytes in necrotic background. Corresponding histopathological section confirms well-formed granulomatous mastitis.
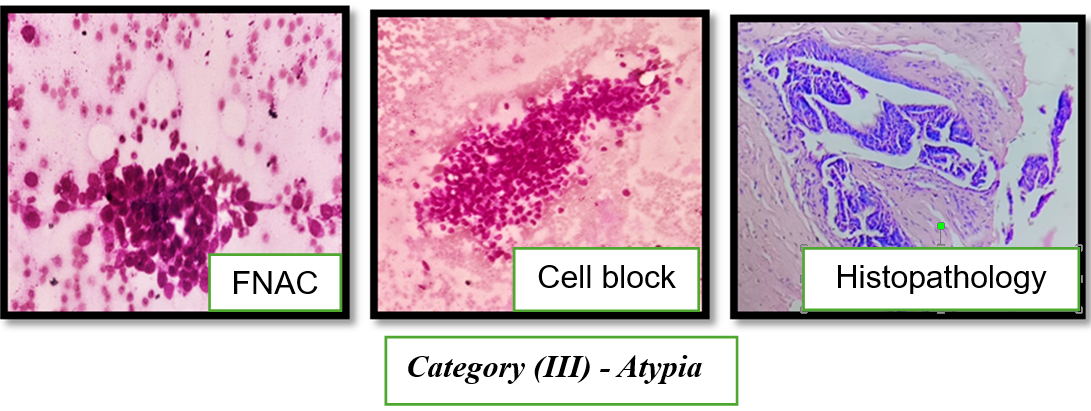
Fig. 3: Fine-needle aspiration cytology features of atypia, probably benign (Category III)
FNAC smears stained with Giemsa show moderately cellular smears composed of crowded epithelial cell clusters with mild architectural disarray and focal nuclear overlapping. On higher magnification, the epithelial cells exhibit mild to moderate cytological atypia with occasional myoepithelial cells in the background. No definite features of malignancy are identified. Cell block preparation shows well-preserved epithelial cell clusters arranged in cohesive patterns withcytological atypia. On Histopathology shows features of atypical ductal hyperplasia.
FNAC results concluded that the majority of the lesions were benign, with 19 cases (63%) classified under Category II (Benign). Among benign lesion the most common tumor diagnosed on FNAC were fibroadenomas (12 cases, 40%), followed by fat necrosis (2 cases, 7%) and galactocele (2 cases, 7%). The FNAC analysis successfully identified these benign lesions with a high level of accuracy.
A total of 3 cases (10%) were categorized as Category III (Atypical), indicating the presence of atypical cells. These cases required further investigation, as FNAC alone could not provide definitive benign or malignant diagnoses. Three cases (10%) contributed in Category IV (Suspicious of Malignancy) group, in which FNAC showed features suggestive of malignancy, such as the presence of atypical epithelial cells. These cases warranted closer examination via the cell block and histopathology to confirm the diagnosis. Four cases (13%) were classified as Category V (Malignant) based on the presence of malignant features and invasive nature in the FNAC aspirates. These diagnoses were consistent with invasive ductal carcinoma, and the malignant nature of these lesions was confirmed by histopathological examination.
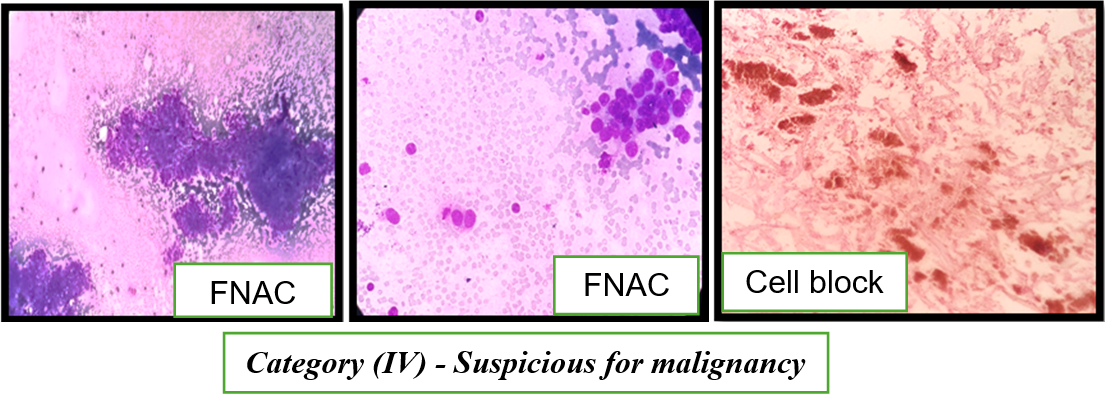
Fig. 4: FNAC findings Suspicious for malignancy (Category IV) showing cohesive and focally discohesive ductal epithelial cell clusters with nuclear enlargement and pleomorphism; cell block inadequate
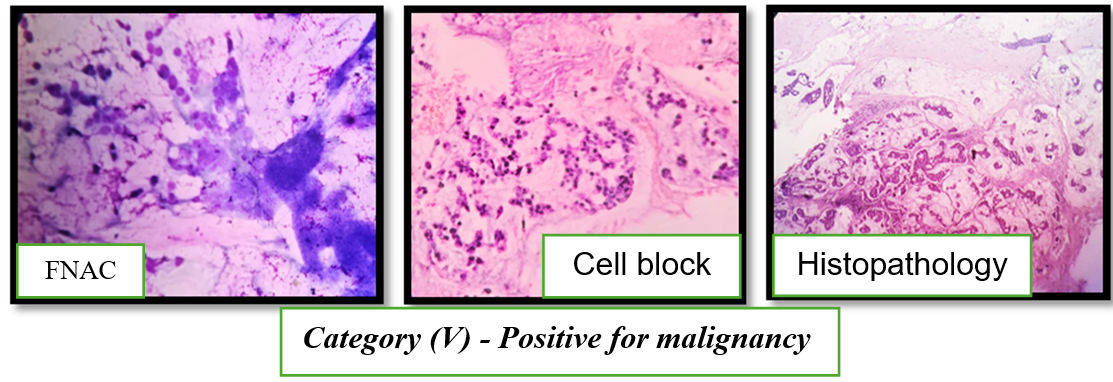
Fig. 5: Fine-needle aspiration cytology, cell block, and histopathological features of mucinous adenocarcinoma of the breast (Category V – Positive for malignancy)
Cell block diagnostic results
FNAC smears show high cellularity with clusters and singly scattered malignant ductal epithelial cells lying in abundant extracellular mucinous background. The tumor cells exhibit marked nuclear atypia, pleomorphism, and hyperchromasia. Cell block sections demonstrate malignant epithelial cell clusters floating within pools of mucin, further supporting the cytological diagnosis. Corresponding histopathological section (HP, 10×) confirms mucinous adenocarcinoma, showing nests and cords of tumor cells embedded in extensive mucin lakes.
The cell block technique provided additional diagnostic information, particularly for cases that were difficult to interpret based solely on FNAC findings. Of the 19 benign cases (63%) identified on FNAC, the cell block confirmed the benign nature in 18 cases, showing clear tissue architecture characteristic of benign lesions such as fibroadenomas, fat necrosis, and gynecomastia. However, one atypical lesion (FNAC Category III) was reclassified as benign after cell block analysis, with evidence of inflammation and fibrosis, further supporting the benign nature of the lesion.
In cases where FNAC was suspicious (Category IV), the cell block provided more definitive results. Three cases categorized as suspicious on FNAC were further examined with cell block preparation. One case showed malignant characteristics, which were consistent with a diagnosis of invasive ductal carcinoma, confirming the malignant nature of the lesion. The other two cases showed benign features upon cell block examination, effectively ruling out malignancy.
Finally, for the 4 cases of malignancy (Category V) identified by FNAC, the cell block confirmed the malignant diagnosis in all instances, identifying features such as malignant ductal cells, pleomorphic nuclei, and mitotic figures, which were consistent with invasive ductal carcinoma. This demonstrated that the cell block technique provided additional histological confirmation and improved diagnostic accuracy in these cases.
Histopathological diagnosis
The histopathological diagnosis, serving as the gold standard for comparison, confirmed the findings of both FNAC and the cell block technique in all cases. Of the 30 patients, the final histopathological diagnoses revealed 19 benign lesions and 8 malignant lesions, with 3 cases requiring additional confirmation through cell block analysis to clarify their benign or malignant nature. The histopathology results were consistent with the cell block findings, with malignant lesions confirmed as invasive ductal carcinoma and other types of malignancies.
The benign lesions confirmed on histopathology included fibroadenomas, fat necrosis, gynecomastia, and galactoceles. The malignant lesions, primarily invasive ductal carcinoma, were diagnosed based on the presence of malignant epithelial cells that exhibited nuclear pleomorphism and mitotic activity.
Effectiveness of combined approach
The combined FNAC and cell block technique showed clear advantages over using either method alone. The most notable improvement was seen in cases that were atypical (Category III) or suspicious (Category IV) in FNAC. In these cases, the cell block provided clearer diagnostic information, enabling better differentiation between benign and malignant lesions. Additionally, the cell block helped confirm inadequate FNAC samples, providing diagnostic clarity in cases where FNAC failed to yield sufficient material.
The combination of these two techniques was particularly beneficial in the suspicious (Category IV) and atypical (Category III) cases. In these categories, FNAC often raised concern but could not provide a definitive diagnosis. The addition of the cell block allowed for better histological evaluation, reducing the number of false positives and false negatives.
Table 1: Study population and lesion characteristics
| Lesion type | Number of cases | Percentage of total |
| Benign lesions | 22 | 73% |
| Malignant lesions | 8 | 27% |
| Fibro adenomas | 12 | 40% |
| Gynecomastia | 1 | 3% |
| Fat necrosis | 2 | 7% |
| Galactocele | 2 | 7% |
| Invasive ductal carcinoma | 8 | 27% |
Table 2: Comparative table: FNAC vs. Cell block diagnostic results
| FNAC category | Lesion type | FNAC number of cases | FNAC percentage | Cell block number of cases | Cell block percentage |
| Category II (Benign) | Acute Mastitis | 2 | 7% | 2 | 7% |
| Granulomatous Lesion | 1 | 3% | 1 | 3% | |
| Galactocele | 2 | 7% | 2 | 7% | |
| Fat Necrosis | 2 | 7% | 2 | 7% | |
| Fibroadenoma | 12 | 40% | 12 | 40% | |
| Gynecomastia | 1 | 3% | 1 | 3% | |
| Category III (Atypical) | Atypical Lesions | 3 | 10% | Inadequate | 0% |
| Category IV (Suspicious) | Suspicious of Malignancy | 3 | 10% | Inadequate | 0% |
| Category V (Malignant) | Malignant Lesions (IDC) | 4 | 13% | 3 | 10% |
Image 1: FNAC diagnostic categories (Total cases and percentages)
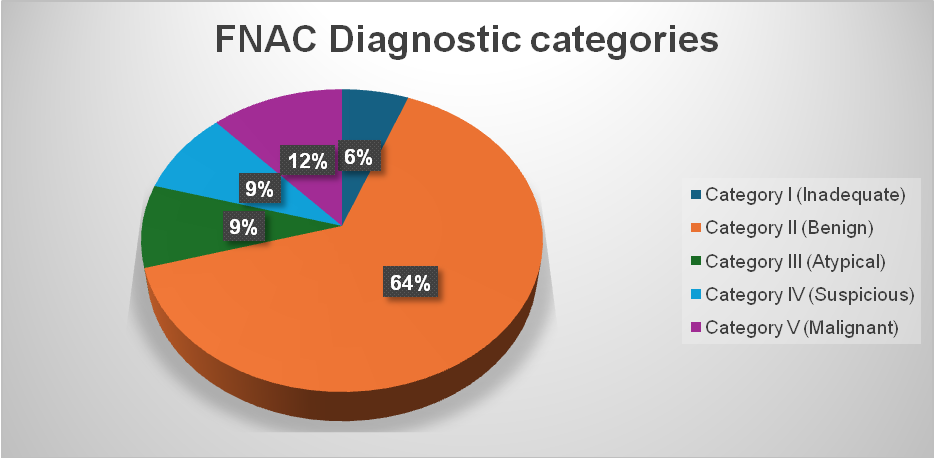
| FNAC category | Number of cases | Percentage |
| Category I (Inadequate) | 2 | 06% |
| Category II (Benign) | 22 | 64% |
| Category III (Atypical) | 3 | 09% |
| Category IV (Suspicious) | 3 | 09% |
| Category V (Malignant) | 4 | 12% |
DISCUSSION
The present study aims to evaluate the diagnostic efficacy of Fine Needle Aspiration Cytology (FNAC) and the cell block technique—both individually and in combination—for the assessment of palpable breast lesions. By incorporating both methods, this study provides valuable insights into their complementary roles in breast pathology diagnostics, especially in a clinical context where prompt and accurate diagnosis is crucial for effective patient management.
FNAC and Its limitations
FNAC has long been established as a minimally invasive, cost-effective, and reliable diagnostic tool for breast lesions. Its ability to provide rapid results with minimal patient discomfort makes it a preferred technique in many clinical settings. In our study, FNAC alone identified benign lesions (Category II) in the majority of cases, with fibroadenoma being the most frequent diagnosis. This observation corroborates prior research, which consistently reports fibroadenoma as the predominant benign lesion in the breast, especially among younger women.
However, while FNAC serves as an effective tool for categorizing most benign and malignant lesions, it does have its limitations. Specifically, FNAC may provide insufficient material in certain cases (Category I-Inadequate), and it often fails to preserve tissue architecture, which is vital for distinguishing between benign and malignant conditions. In our study, 9% of the cases were categorized as suspicious (Category IV), and 10% were atypical (Category III), both of which are categories that present diagnostic challenges and necessitate further investigation or confirmation. These findings are consistent with the limitations of FNAC reported by other studies, where the accuracy of FNAC in diagnosing atypical or suspicious lesions has been found to be lower than in the evaluation of clearly benign or malignant lesions.
The role of cell block technique
The cell block technique has become an important adjunct to FNAC due to its ability to preserve tissue architecture, which is critical in the evaluation of complex lesions. In our study, the use of cell block preparations significantly improved diagnostic accuracy, especially in categories where FNAC alone provided inconclusive results. Cell blocks allow for better visualization of tissue structure and can be used for additional testing, such as immunohistochemistry (IHC), molecular studies (e. g., PCR, FISH), and gene expression profiling. This is particularly useful in cases of granulomatous lesions, suspected malignancies, and atypical lesions, where precise categorization is crucial for determining the correct clinical course.
Histopathological correlation and clinical implications
In our study, histopathological evaluation of the excised tissue served as the gold standard for confirming the diagnosis. The correlation between FNAC and histopathology was strong for benign lesions, including fibroadenomas, fat necrosis, and mastitis. However, in cases classified as Category III (atypical) or Category IV (suspicious), cell block preparations were more useful in providing conclusive evidence. For instance, a case of fibroadenoma that was initially classified as atypical in FNAC was confirmed as benign upon cell block analysis, providing an additional layer of diagnostic certainty.
Moreover, the combination of FNAC and cell block helped in cases where FNAC alone could not provide definitive results due to haemorrhage, insufficient material, or inadequate cellularity. This highlights a key advantage of the combined approach: it provides multiple diagnostic angles, improving the overall diagnostic yield, particularly in difficult-to-diagnose cases. Such cases are common in clinical practice, where FNAC may yield inconclusive results, but the additional tissue from cell block preparations can offer a more comprehensive diagnosis.
Study limitations and areas for improvement
Despite its advantages, the cell block technique also has its limitations. In our study, several samples from malignant or suspicious cases were inadequate due to haemorrhagic aspirates or low cellularity, which is consistent with findings from previous studies. This issue emphasizes the importance of meticulous sampling techniques and optimal fixation methods to ensure the success of the cell block technique. Furthermore, the small sample size in our study (30 cases with both FNAC and cell block analysis) may limit the generalizability of the findings, and larger cohort studies are needed to validate these results on a broader scale.
CONCLUSION
This study demonstrates that combining FNAC with the cell block technique significantly enhances diagnostic accuracy for breast lesions, particularly in cases that are difficult to diagnose on FNAC alone. The combination of these two techniques allows for a more comprehensive evaluation, providing detailed architectural features and the opportunity for additional testing, such as immunohistochemistry and molecular assays. In clinical practice, this approach offers a cost-effective, minimally invasive, and reliable diagnostic pathway for the management of breast lesions, helping to guide clinical decision-making and reduce the need for more invasive procedures. The results of this study align with previous research suggesting that the combined approach of FNAC and cell block should be considered as a standard practice in breast pathology, especially in settings where rapid and accurate diagnosis is essential for better prognoses.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
CONFLICT OF INTERESTS
Declared none
REFERENCES
Daramola AO, Odubanjo MO, Obiajulu FJ, Ikeri NZ, Banjo AA. Correlation between fine-needle aspiration cytology and histology for palpable breast masses in a Nigerian tertiary health institution. Int J Breast Cancer. 2015;2015:742573. doi: 10.1155/2015/742573, PMID 26635977.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011 Mar-Apr;61(2):69-90. doi: 10.3322/caac.20107.
Stewart BW, Wild CJ; WHO. World cancer report 2014. Lyon, France: International Agency for Research on Cancer; 2014. Available from: https://publications.iarc.fr/non-series-publications/world-cancerreports/world-cancer-report-2014.
Malvia S, Bagadi SA, Dubey US, Saxena S. Epidemiology of breast cancer in Indian women. Asia Pac J Clin Oncol. 2017;13(4):289-95. doi: 10.1111/ajco.12661, PMID 28181405.
Prakash D, Puvvala ORK, Nuguri VK, Priyanka V. Advantages of the cell block technique over the FNAC and correlation with histopathology of most prevalent breast lesions in the community at the tertiary care center. Indian J Pathol Oncol. 2022;9(4):315-7. doi: 10.18231/j.ijpo.2022.075.
Basnet S, Talwar OP. Role of cell block preparation in neoplastic lesions. J Pathol Nep. 2012;2(4):272-6. doi: 10.3126/jpn.v2i4.6876.
Ashwinkumar KB, Pradeep U, Archana D, Pradeep M, Ahilya D, Ajay J. Diagnostic utility of cell block preparation of fine needle aspiration material. SJAMS. 2017;5(12):5031-7. doi: 10.36347/sjams.2017.v05i12.048.
Hegazy RA. Fine needle aspiration cytology and cell-block study of various breast lumps. AJBLS. 2014;2(1):8. doi: 10.11648/j.ajbls.20140201.12.
Jatin Patel M, C Patel S. Fine needle aspiration cytology and cell block study of various breast lumps. J Cytol Histol. 2018;9(4):514. doi: 10.4172/2157-7099.1000514.
Kawatra S, Sudhamani S, Kumar SH, Roplekar P. Cell block versus fine-needle aspiration cytology in the diagnosis of breast lesions. J Sci Soc. 2020;47(1):23-7. doi: 10.4103/jss.JSS_12_20.