
Int J Curr Pharm Res, Vol 18, Issue 2, 112-117Original Article
COMPARISON OF ULTRASOUND GUIDED ERECTOR SPINAE PLANE BLOCK AND LOCAL SKIN INFILTRATION FOR POSTOPERATIVE ANALGESIA IN ADULT PATIENTS UNDERGOING LUMBAR SPINE SURGERY UNDER GENERAL ANAESTHESIA
MANSI MITTAL1, CHANDANDEEP KAUR2*
¹Department of Anesthesia, Medanta-The Medicity, Gurugram, Haryana, India. ²Department of Anesthesia, Government Medical College, Patiala, Punjab, India
*Corresponding author: Chandandeep Kaur; *Email: drckdhanoa@gmail.com
Received: 14 Nov 2025, Revised and Accepted: 01 Jan 2026
ABSTRACT
Objective: To compare the efficacy of ultrasound-guided Erector Spinae Plane (ESP) block with local skin infiltration for postoperative analgesia in adult patients undergoing lumbar spine surgery under general anaesthesia.
Methods: Sixty ASA I-II patients aged 18-80 y undergoing elective lumbar spine surgery were randomized into two groups of 30 each. Group E received ultrasound-guided bilateral ESP block with 0.25% Bupivacaine 10 ml on each side (total 20 ml), while Group l received local skin infiltration with 20 ml of 0.25% Bupivacaine. Visual Analogue Scale (VAS) scores, time to first rescue analgesia, hemodynamic parameters (heart rate, blood pressure, mean arterial pressure, SpO2), and adverse effects were assessed at 15 min, 30 min, 1 h, 1.5 h, 2 h, 4 h, and 6 h postoperatively.
Results: Group E demonstrated significantly lower VAS scores at all time intervals compared to Group l (p<0.05). The time to first rescue analgesia was significantly prolonged in Group E (1.95±0.48 h) compared to Group l (1.63±0.43 h, p=0.01). Group E showed better hemodynamic stability with significantly lower pulse rate and mean arterial pressure at 6 h (p<0.05). SpO2 was significantly higher in Group E at 15 min, 30 min, 2 h, and 4 h (p<0.05). No adverse effects were observed in either group.
Conclusion: Ultrasound-guided erector spinae plane (ESP) block provides superior postoperative analgesia, prolongs the time required for rescue analgesia, reduces opioid consumption, and maintains better hemodynamic stability compared to local skin infiltration in patients undergoing lumbar spine surgery.
Keywords: Erector spinae plane block, Local skin infiltration, Postoperative analgesia, Lumbar spine surgery, Ultrasound-guided, Bupivacaine, Visual analogue scale, Rescue analgesia
© 2026 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/)
DOI: https://dx.doi.org/10.22159/ijcpr.2026v18i2.8075 Journal homepage: https://innovareacademics.in/journals/index.php/ijcpr
INTRODUCTION
Spine disorders are one of the most frequently encountered problems in clinical medicine. Lumbar spinal surgeries are widely accepted as surgical treatment for various spinal disorders [1, 2] and with the introduction of minimally invasive procedures, there has been an increase in the number of spine procedures [3]. Rate of hospitalizations increased more than 33% in each sex, with that of lumbar fusion surgery increasing more than 60% in each sex [4]. Spinal surgeries usually cause intense and severe pain as they involve the dissection of subcutaneous tissue, bones and ligaments. Maximum pain occurs in the first 4 postoperative hours and gradually declines in the third postoperative day [5]. Postoperative pain can lead to complications like delayed mobilization, pulmonary and thromboembolic complications, prolonged hospital stay and chronic pain syndromes and therefore efficient and safe methods for postoperative analgesia are required after lumbar spine surgeries.
Conventional techniques for pain management include use of opioids, NSAIDS, epidural analgesia and local skin infiltration. Local infiltration analgesia is safe, simple and provides effective management for postoperative pain in lumbar spine surgeries [6]. Rare side effects include orthostatic hypotension, nausea and vomiting. New regional anaesthetic techniques such as the Erector Spinae Plane block, are being studied for the purpose of spine surgeries to provide better pain relief. Ultrasound availability has improved the safety and efficacy of regional anaesthesia and helps in confirming the deposition of local anaesthetic drugs in the correct plane safely. Due to ease of application, low complications rates, effective postoperative analgesia and reduction of opioid consumption, these blocks are being frequently employed [7].
The Erector Spinae Plane (ESP) block was recently discovered by Forero and colleagues in 2016 [8]. It is a paraspinal interfascial block targeting ventral and dorsal rami of spinal nerves. Its key advantage is the multilevel spread of local anaesthetics in the fascial plane by a single injection. It is performed away from the spinal cord, has procedural simplicity and minimal complications and is therefore chosen for postoperative analgesia of spine surgeries.
MATERIALS AND METHODS
After obtaining approval from Institutional Ethical Committee and prior written informed consent from all the patients, sixty patients of ASA grades 1 and 2 of either sex, in the age group 18-80 y who were undergoing elective lumbar spine surgery under general anaesthesia requiring postoperative analgesia were enrolled for this randomized comparative study.
Patients with pre-existing coagulation disorders, local infection at the site of injection and with allergy to Bupivacaine were excluded from the study. Subjects were randomized to one of the two groups of 30 each. A complete pre-anaesthetic evaluation was performed in each patient. The patient received tablet al. prazolam 0.25 mg one night prior to the day of surgery. Patients were randomly selected between two groups by random number generating function.
Group L: Patients received 20 ml of 0.25% Bupivacaine by local skin infiltration technique.
Group E: Patients received ultrasound-guided ESP block with 0.25% Bupivacaine 10 ml on each side (Total-20 ml).
After receiving the patient in the operation theatre, Electrocardiogram (ECG), Non Invasive Blood Pressure (NIBP) were recorded and pulse oximeter was attached and baseline parameters were recorded. After securing an IV line with 18G cannula in a large peripheral vein of hand, preloading was done with RL solution 15 ml per kg body weight which was infused over 15 min. Anaesthesia machine, airway equipment were checked and drugs for resuscitation and general anaesthesia were kept ready before starting the procedure. After premedication with injection Midazolam 1 mg iv, induction with propofol 2 mg/kg plus fentanyl 1.5mcg/kg and muscle relaxant with injection vecuronium bromide 0.1 mg/kg were given. Intermittent Positive Pressure Ventilation was done with oxygen, nitrous oxide and sevoflurane. After Intubation, anaesthesia was maintained with sevoflurane and intermittent doses of injection vecuronium bromide. Duration of surgery varied between 45 min to 1.5 h. Vitals monitoring was done and at the end of the surgery depending on the group allocated to the patient corresponding procedure was done using 0.25% Bupivacaine. Procedure was done under all aseptic precautions.
Group L: Local skin infiltration technique-After completion of surgery 20 ml of 0.25% Bupivacaine was infiltrated under vision into the tissues.
Group E: Ultrasound guided ESP block-After the surgery, spine was palpated downwards from C7 to T10 and T10 was marked. A linear USG probe of high frequency was taken and covered with sterile transparent dressing and sterile conductivity gel was applied. The probe was placed longitudinally in the midline at T10 level. Spinous process was visualized, after which probe was lateralized, and the transverse processes and erector spinae muscle were seen approximately 3 cm laterally to the midline. The skin was then infiltrated with LA and 22G, 80 mm special needle for USG guided block was used. The tip of the needle was advanced under direct visualisation until it was placed into the fascial plane on the deep aspect of erector spinae muscle. The correct location of the needle was confirmed by visible fluid spread below the erector spinae muscle off the bony shadow of the transverse process. A total volume of 10 ml of 0.25% Bupivacaine was injected through the needle after aspiration. The procedure was then repeated on the opposite side with 10 ml of 0.25% Bupivacaine.
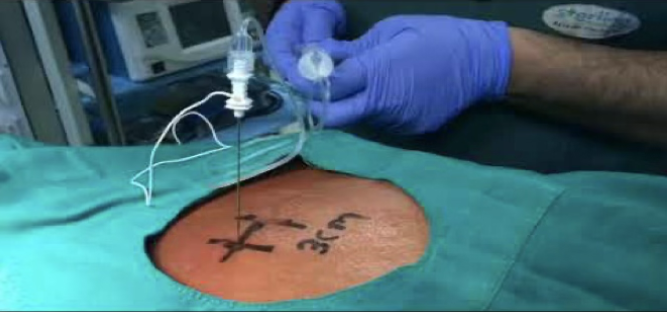
Fig. 1: Ultrasound-guided erector spinae plane block
After the completion of the procedure the patient was reversed with 0.05 mg/kg injection of Neostigmine and 0.01 mg/kg injection of glycopyrrolate and then extubation was done. After stabilization, the patient was shifted to the recovery room for post-operative monitoring.
Multimodal analgesia was given for pain management. For all patients we gave injection paracetamol 1g iv 1 h prior to the end of surgery and then the corresponding procedure was performed to the allotted groups on completion of surgery. The following parameters were assessed in the recovery room:
-The duration of analgesia was assessed by time between the administration of block and time of first rescue analgesia dose at intervals of 15 min, 30 min, 1h, 1.5 h, 2h, 4 h and 6h. Inj Tramadol 1 mg/kg was given as the first rescue analgesic dose when VAS is more than 4.
-The hemodynamic parameters like heart rate (HR), Blood pressure (BP), mean Arterial Pressure (MAP) and saturation between the two procedures were measured at same time intervals as said above.
-Adverse effects like hypotension, nausea and vomiting if any were recorded.
RESULTS AND OBSERVATION
In the present study, the groups were comparable with respect to demographic characteristics, anthropometric parameters, comorbidities and baseline parameters.
Table 1: Comparison of visual analogue score between group E and L
| Visual analogue score | Group E(n=30) | Group L(n=30) | Total | P value |
| 15 min | ||||
| Mean±SD | 1.87±0.73 | 2.93±0.58 | 2.4±0.85 | <.0001* |
| Median (25th-75th percentile) | 2(1-2) | 3(3-3) | 2(2-3) | |
| Range | 1-4 | 2-4 | 1-4 | |
| 30 min | ||||
| Mean±SD | 2.27±0.64 | 3.57±0.57 | 2.92±0.89 | <.0001* |
| Median (25th-75th percentile) | 2(2-3) | 4(3-4) | 3(2-4) | |
| Range | 1-4 | 3-5 | 1-5 | |
| 1 h | ||||
| Mean±SD | 3.3±0.7 | 3.9±0.76 | 3.6±0.79 | 0.002* |
| Median (25th-75th percentile) | 3(3-4) | 4(3-4) | 3.5(3-4) | |
| Range | 2-5 | 3-6 | 2-6 | |
| 1.5 h | ||||
| Mean±SD | 4.2±0.96 | 4.87±0.97 | 4.53±1.02 | 0.01* |
| Median (25th-75th percentile) | 4(3.25-5) | 5(4-6) | 4(4-5) | |
| Range | 3-6 | 3-7 | 3-7 | |
| 2 h | ||||
| Mean±SD | 4.9±0.76 | 6.37±0.76 | 5.63±1.06 | <.0001* |
| Median (25th-75th percentile) | 5(5-5) | 6(6-7) | 6(5-6) | |
| Range | 3-6 | 5-8 | 3-8 | |
| 4 h | ||||
| Mean±SD | 6.1±0.55 | 6.73±0.91 | 6.42±0.81 | 0.002* |
| Median (25th-75th percentile) | 6(6-6) | 7(6-7) | 6(6-7) | |
| Range | 5-8 | 5-9 | 5-9 | |
| 6 h | ||||
| Mean±SD | 7.5±0.57 | 8.2±0.61 | 7.85±0.68 | <.0001* |
| Median (25th-75th percentile) | 7(7-8) | 8(8-9) | 8(7-8) | |
| Range | 7-9 | 7-9 | 7-9 |
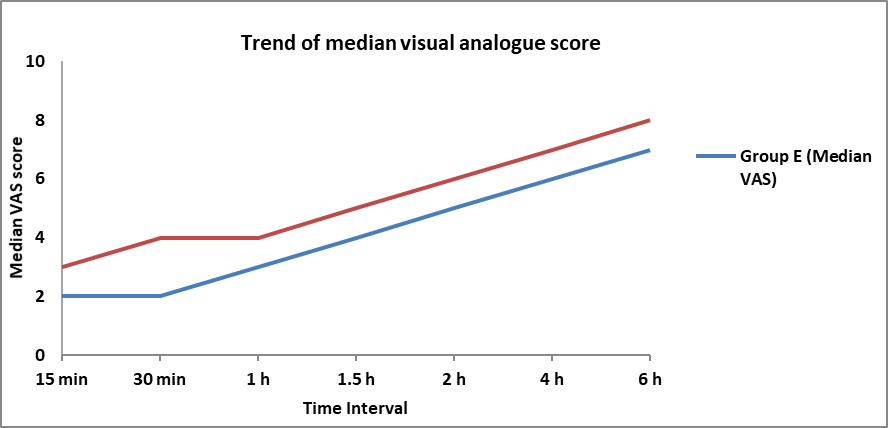
Fig. 2: Comparison of trend of visual analogue score at different time intervals between group E and L
Mean±SD of visual analogue score 15 min, 30 min, 1 h, 1.5 h, 2 h, 4 h, 6 h in group l was 2.93±0.58, 3.57±0.57, 3.9±0.76, 4.87±0.97, 6.37±0.76, 6.73±0.91, 8.2±0.61 respectively which was significantly higher as compared to group E 1.87±0.73 (p value<.0001), 2.27±0.64 (p value<.0001), 3.3±0.7 (p value=0.002), 4.2±0.96 (p value=0.01), 4.9±0.76 (p value<.0001), 6.1±0.55 (p value=0.002), 7.5±0.57 (p value<.0001)) respectively.
No significant difference was seen in post-operative SpO2 (%) at 1 h (p value=0.174), 1.5 h (p value=0.802), 6 h (p value=0.553) between group E and L. mean±SD of post-operative SpO2 (%) at 1 h, 1.5 h, 6 h in group E was 99.77±0.43, 99.77±0.43, 99.53±0.68 respectively and in group l was 99.53±0.82, 99.73±0.58, 99.63±0.61 respectively with no significant difference between them.
Table 2: Comparison of rescue analgesia (hours) between group E and L
| Rescue analgesia (hours) | Group E(n=30) | Group L(n=30) | Total | P value |
| Mean±SD | 1.95±0.48 | 1.63±0.43 | 1.79±0.48 | 0.01* |
| Median(25th-75th percentile) | 2(1.5-2) | 1.5(1.5-2) | 1.75(1.5-2) | |
| Range | 1.5-3 | 1-3 | 1-3 |
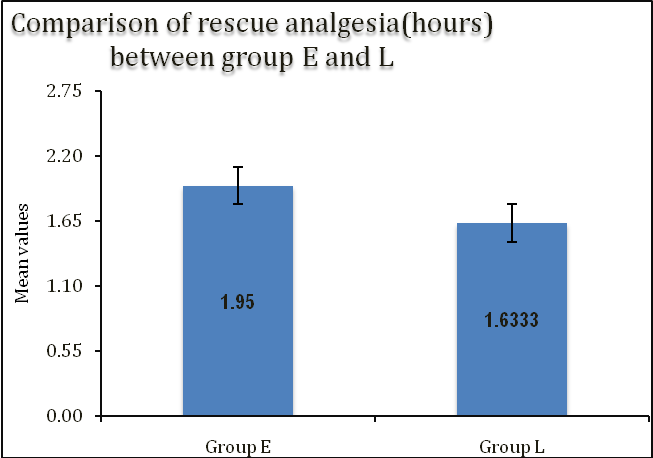
Fig. 3: Comparison of rescue analgesia (hours) between group E and L., mean±SD of rescue analgesia (hours) in group E was 1.95±0.48 which was significantly higher as compared to group l 1.63±0.43 (p value=0.01))
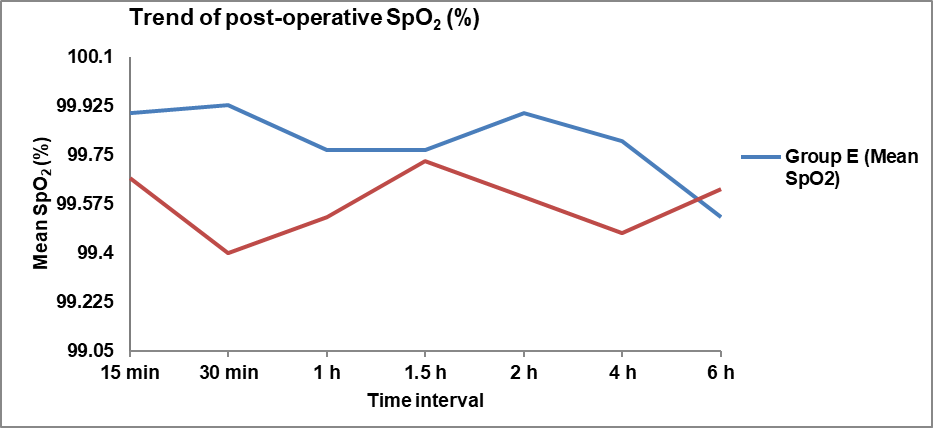
Fig. 4: Comparison of trend of post-operative SpO2 (%) at different time intervals between group E and L, mean±SD of post-operative SpO2 (%) at 15 min, 30 min, 2 h, 4 h in group E was 99.9±0.31, 99.93±0.25, 99.9±0.31, 99.8±0.41 respectively which was significantly higher as compared to group l (99.67±0.48 (p value=0.029), 99.4±0.77 (p value=0.001), 99.6±0.67 (p value=0.032), 99.47±0.73 (p value=0.034)) respectively
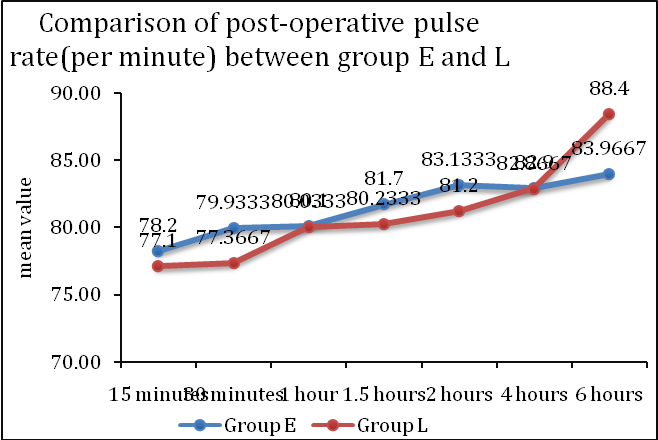
Fig. 5: Comparison of trend of post-operative pulse rate (per minute) at different time intervals between group E and L, mean±SD of post-operative pulse rate (per minute) at 6 h in group l was 88.4±3.4 which was significantly higher as compared to group E (83.97±6.32 (p value=0.001))
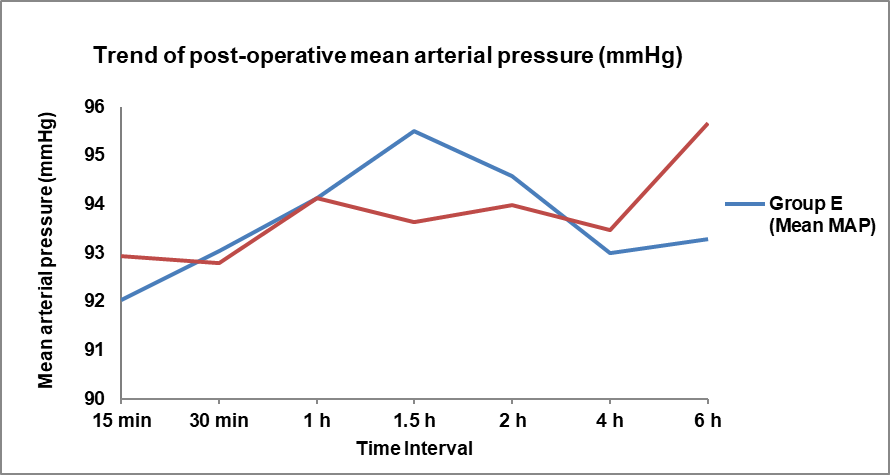
Fig. 6: Comparison of trend of post-operative mean arterial pressure (mmHg) at different time intervals between group E and L
No significant difference was seen in post-operative pulse rate (per minute) at 15 min (p value=0.485), 30 min (p value=0.086), 1 h (p value=0.964), 1.5 h (p value=0.291), 2 h (p value=0.113), 4 h (p value=0.98) between group E and L. mean±SD of post-operative pulse rate (per minute) at 15 min, 30 min, 1 h, 1.5 h, 2 h, 4 h in group E was 78.2±5.9, 79.93±5.58, 80.1±5.9, 81.7±6.19, 83.13±5.64, 82.9±6 respectively and in group l was 77.1±6.21, 77.37±5.81, 80.03±5.37, 80.23±4.3, 81.2±3.36, 82.87±4.17 respectively with no significant difference between them.
No significant difference was seen in post-operative systolic blood pressure at any interval. For postoperative diastolic blood pressure, mean±SD at 6 h in group l was 82.17±5.95 which was significantly higher as compared to group E (78.97±4.86 with p-value 0.026). At other intervals, no significant difference was seen between the two groups with respect to DBP.
Mean±SD of post-operative mean arterial pressure (mmHg) at 6 h in group l was 95.67±5.18 which was significantly higher as compared to group E (93.27±4.01 (p value=0.049)).
No significant difference was seen in post-operative mean arterial pressure (mmHg) at 15 min (p value=0.459), 30 min (p value=0.841), 1 h (p value=1), 1.5 h (p value=0.053), 2 h (p value=0.54), 4 h (p value=0.604) between group E and L. Mean±SD of post-operative mean arterial pressure (mmHg) at 15 min, 30 min, 1 h, 1.5 h, 2 h, 4 h in group E was 92.03±4.16, 93.03±5.22, 94.13±5.32, 95.5±4.18, 94.57±4.29, 93±3.91 respectively and in group l was 92.93±5.13, 92.78±4.6, 94.13±3.07, 93.63±3.02, 93.97±3.17, 93.47±2.96 respectively with no significant difference between them.
Adverse events did not occur in any of the patients in both the groups.
DISCUSSION
Pain management is one of the most important components of optimal postoperative care. With the introduction of USG, peripheral nerve blocks are increasingly being used for postoperative pain relief. Ultrasound-guided Erector Spinae Plane (ESP) block, introduced recently in 2016, had promising results in controlling postoperative pain. In our study, we compared postoperative analgesia in patients undergoing lumbar spine surgery under GA by USG guided ESP block and local infiltration.
In our study, the time of rescue analgesia in Group E was 1.95±0.48 h and in Group l was 1.63±0.43 h. We observed in our study that the time required for rescue analgesic dose was prolonged in Group E Patients as compared to Group L. This is in agreement with study by Yayik AM, Cesur S, Ozturk F, Ahiskalioglu A, Ay AN, Celik EC, Kilinc A [9], on 60 patients undergoing lumbar decompression surgery for postoperative efficacy of ultrasound-guided ESP block. Patients were randomly assigned into 2 groups. One group received a usg-guided bilateral ESP block with 0.25% Bupivacaine 20 ml. In the control group, no intervention was performed. Results showed that the time to first rescue analgesic requirement was significantly longer in the ESP group than in the control group (p<0.05). Wang Q, Zhang G, Wei S, He Z, Sun L, Zheng H [10], on the efficacy of ESP block versus wound infiltration for postoperative pain in patients undergoing thoracotomy on 60 patients using 20 ml of 0.5% ropivacaine who reported a statistically significant difference in postoperative opioid consumption between the two groups (p<0.05). Our study results correlated well with these studies.
Vas score (Quality of analgesia)
Quality of the analgesia was assessed by the VAS (Visual Analog Score) after the arrival of the patient in the recovery room at 15 min, 30 min, 1, 1.5, 2, 4 and 6 h from the time of procedure done and also as and when the patient complains of the pain.
In our study, the VAS score was compared between group E (ultrasound-guided erector Spinae Plane block) and group l (local infiltration of anaesthesia). In Group E after 15 min mean VAS score was 1.87±0.73 and in group l 2.93±0.58 with p value of less than 0.0001, after 30 min group E had mean VAS score of 2.27±0.64 whereas group l showed 3.57±0.57 with p value<0.0001, after 1h group E had mean VAS score of 3.3±0.7 whereas group l had 3.9±0.76 with p value<0.002, after 1.5 h group E showed mean VAS of 4.2±0.96 and group l showed 4.87±0.97 with p value<0.01, after 2 h group E showed mean VAS of 4.9±0.76 whereas group l had 6.37±0.76 with p value<0.0001, after 4 h group E showed mean VAS of 6.1±0.55 whereas group l had 6.73±0.91 with p value less than 0.002 and after 6 h group E had mean VAS of 7.5±0.57 and in group l showed 8.2±0.61 with p-value<0.0001. Our study results were statistically significant at all intervals. We found in our study that Group E had better post-operative analgesic outcome with respect to dose of rescue analgesia requirement, in comparison to Group L.
Singh S, Chaudhary NK [11] conducted a study on 40 patients undergoing lumbar spine surgery to study post-operative analgesic effect of ultrasound guided Erector Spinae Plane block with a control group using 20 ml of 0.5% bupivacaine. Results showed that pain scores immediately after surgery (p=0.002) and after 6 h after surgery (p=0.040) were lower in the ESP block group. Patient satisfaction scores were more favourable in the block group (p<0.0001).
Adhikary SD, Liu WM, Fuller E, Cruz-Eng H, Chin KJ [12] conducted a retrospective study to study the effectiveness of bilateral ultrasound-guided Erector Spinae Plane block (ESPB) in percutaneous lumbar osteosynthesis for spine trauma. Some patients received preoperative bilateral ESPB (30 ml of 0.375% ropivacaine) on each side, others received the standard of care i. e., postoperative muscular infiltration with the same amount of drug. The primary outcome was the cumulative morphine consumption at 24 h postoperatively. Secondary outcomes included pain scores at various time points until 24 h. Postoperative VAS scores in Group ESP were significantly reduced at 30 min, 1st h, 1 h 30 min, 2, 4, and 6 h (P<0.001). The VAS scores in the control group were high from the beginning of 30 min to 6 h when compared to the ESP group.
Our study results showed that Group E patients who received Erector Spinae block had an overall reduction of the analgesic requirement in the post-operative period which is comparable with the above studies.
Vital parameters comparison: post-operative
In our study, we also compared hemodynamic parameters like pulse rate, mean arterial blood pressure and saturation between Group E and Group l in the same intervals as observed for VAS score.
Group E had less post-operative pulse rate than compared to group l which is statistically significant at the interval of 6th h with p value of 0.001 and at 15 min, 30 min, 1 h, 1.5 h, 2 h and 4 h it was almost equal with no significance.
Group E had less mean arterial blood pressure in comparison to Group l which is statistically significant at 6 h with p value of 0.049 and at other intervals, it was almost equal in both the groups.
The lower pulse rate and mean arterial blood pressure in Group E is due to better analgesia.
Adverse effects
In our study, no adverse effects like post-operative nausea and vomiting were observed in either of the groups, which correlated with the previous study.
LIMITATIONS
There were a few limitations in our study. The small sample size was one of the limitations of our study. A small study population precluded the conclusion about failure rate and complications. So further studies need to be undertaken with a large sample size.
Secondly, in our study, the technique for providing analgesia was administered postoperatively, but if it was given preoperatively, it would have decreased the intraoperative pain also thereby benefitting the patient. We did not compare the total analgesic requirement in both groups for 24 h, which could have an impact on the study.
CONCLUSION
There has been an increasing trend in the number of spine procedures worldwide. However, these surgeries are associated with intense pain and discomfort in the postoperative period. Various techniques are used to alleviate pain in postoperative period in spine surgeries like the use of opioids, NSAIDs, epidural analgesia and local skin infiltration. Local skin infiltration was found effective in relieving postoperative pain. Ultrasound-guided Erector Spinae Plane (ESP) block is also being effectively used as a postoperative analgesic treatment method for various surgeries. Hence in our present study, we had compared the above two techniques i. e. ESP block and local skin infiltration for postoperative pain management in lumbar spine surgery patients. The findings of this study indicate that Ultrasound-guided Erector Spinae Plane (ESP) block provides better postoperative analgesia, prolongs the time required for rescue analgesia, thereby decreasing the need for further opioid consumption while maintaining better hemodynamic stability than skin infiltration of local anaesthesia in patients undergoing lumbar spine surgery.
FUNDING
Nil
AUTHORS CONTRIBUTIONS
All authors have contributed equally
CONFLICT OF INTERESTS
Declared none
REFERENCES
Provaggi E, Capelli C, Leong JJ, Kalaskar DM. A UK-based pilot study of current surgical practice and implant preferences in lumbar fusion surgery. Med (Baltim). 2018;97(26):e11169. doi: 10.1097/MD.0000000000011169, PMID 29952965.
Mobbs RJ, Phan K, Malham G, Seex K, Rao PJ. Lumbar interbody fusion: techniques indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J Spine Surg. 2015;1(1):2-18. doi: 10.3978/j.issn.2414-469X.2015.10.05, PMID 27683674.
Reisener MJ, Pumberger M, Shue J, Girardi FP, Hughes AP. Trends in lumbar spinal fusion-a literature review. J Spine Surg. 2020;6(4):752-61. doi: 10.21037/jss-20-492, PMID 33447679.
Davis H. Increasing rates of cervical and lumbar spine surgery in the United States, 1979-1990. Spine. 1994;19(10):1117-23. doi: 10.1097/00007632-199405001-00003, PMID 8059266.
Bianconi M, Ferraro L, Traina GC, Zanoli G, Antonelli T, Guberti A. Pharmacokinetics and efficacy of ropivacaine continuous wound instillation after joint replacement surgery. Br J Anaesth. 2003;91(6):830-5. doi: 10.1093/bja/aeg277, PMID 14633754.
Saini D, Yadav U. Study of wound instillation technique for effective postoperative analgesia using ropivacaine in lumbar spine surgery. Anesth Essays Res. 2018;12(3):685-9. doi: 10.4103/aer.AER_87_18, PMID 30283176.
Chin KJ, McDonnell JG, Carvalho B, Sharkey A, Pawa A, Gadsden J. Essentials of our current understanding: abdominal wall blocks. Reg Anesth Pain Med. 2017;42(2):133-83. doi: 10.1097/AAP.0000000000000545, PMID 28085788.
Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42(3):372-6. doi: 10.1097/AAP.0000000000000581, PMID 28272292.
Yayik AM, Cesur S, Ozturk F, Ahiskalioglu A, Ay AN, Celik EC. Postoperative analgesic efficacy of the ultrasound-guided erector spinae plane block in patients undergoing lumbar spinal decompression surgery: a randomized controlled study. World Neurosurg. 2019;126:e779-85. doi: 10.1016/j.wneu.2019.02.149, PMID 30853517.
Wang Q, Zhang G, Wei S, He Z, Sun L, Zheng H. Comparison of the effects of ultrasound-guided erector spinae plane block and wound infiltration on perioperative opioid consumption and postoperative pain in thoracotomy. J Coll Physicians Surg Pak. 2019;29(12):1138-43. doi: 10.29271/jcpsp.2019.12.1138, PMID 31839083.
Singh S, Chaudhary NK. Bilateral ultrasound guided erector spinae plane block for postoperative pain management in lumbar spine surgery: a case series. J Neurosurg Anesthesiol. 2019;31(3):354. doi: 10.1097/ANA.0000000000000518, PMID 29965831.
Adhikary SD, Liu WM, Fuller E, Cruz-Eng H, Chin KJ. The effect of erector spinae plane block on respiratory and analgesic outcomes in multiple rib fractures: a retrospective cohort study. Anaesthesia. 2019;74(5):585-93. doi: 10.1111/anae.14579, PMID 30740657.